Hi all, we had a giant COVID-19 Conference last week. I want to make sure that everybody has a chance to review the content that was shared!
EM/ICU COVID Panel
A huge thank you to all of our guests who joined us for the EM/ICU panel. Below you can find the video as well as a summary of the discussion that was being had on the chatroom!
Our very own Dr. Blaine White took a DEEP dive into COVID. He made a very well written document that dives into COVID-19, how the virus works, and how we might stop it.
We were also joined last week by our very own PharmD Rachel Wein. See all of the material below for you to review. I have also added an additional video on making push dose pressors as well as the guide that Dr. Franckowiak put together for you!
Hi all, see below for even more resources on COVID-19. Dr. Darr put together another great summary of resources for airway considerations. Also, didn’t want to forget posting Dr. Jano’s great lecture on charts/RVUs, when we survive the coronapocalypse we gotta get paid for those level 5 charts
Hi all, as you know times are weird right now with COVID-19. We will update you ASAP regarding any conference cancellations so stay tuned. First and foremost. The wonderful Dr. Darr has put together a great power point that links the high yield resources and gives an overview of the disease
For conference, we will be covering esophageal/stomach pathology and GI bleeds. There will be a great hands on procedure station for using blakemore tubes. PLEASE review the required content below. We want everyone to be able to practice this as it is QUITE rare to do.
Welcome to the final block of Cardiology. This week will cover all things valvular and clot related in the ED. Special guests include Dr. Lieberman to talk about cardiogenic syncope and Dr. Griffiths to talk about pulmonary hypertension. Also we will have a wellness discussion on sleep and diet, followed by an admin lecture by Dr. Berk.
Eastman CI, Stewart KT, Mahoney MP, et al. Dark goggles and bright light improve circadian rhythm adaptation to night-shift work. Sleep. 1994 Sep;17(6):535-43. PMID 7809567
Kuhn G. Circadian rhythm, shift work, and emergency medicine. Ann Emerg Med. 2001 Jan;37(1):88-98. PMID 11145778 Brewster J.
Nutrition:
Beginning Nutrition: The Facts About Protein, Carbs & Fat. Bodybuilding.com website. https://www.bodybuilding.com/content/beginning- nutrition-the-facts-about-protein-carbs-fat.html. January 1, 2016. Accessed August 6, 2017.
Hey all! Now that Inservice is behind us we will resume our normally scheduled conferences. We still have TWO more cardio blocks to finish up (for the record we are on pt 4/5). This week we will have Dr. Nangia Jr teaching us about endocarditis/myocarditis, a deep dive into PEA arrest by Dr. White, as well as a megacode sim station run by Dr. Saker.
Dr. White’s deep dive: PLEASE, take the time to study the REQUIRED MATERIAL below. The deep dive station will be a true FLIP and require your participation.
Big Tuna’s Megacode: This will involve running through several cardiac arrest cases in pseudo-sim fashion. We will have ED nurses there to help out. The aim will be for the interns to practice LEADING codes, and for the 2nd/3rd years to assist.
FYI no quiz this week… we are taking a quiz break since we are post inservice
Hey team, hope you are all studying hard. We are in the final stretch for the inservice. We had a lot of great review content the past couple weeks. Unfortunately, we cannot share Dr. Wollman’s review (it is his patented educational child). However enjoy the wealth of other study material below. Make sure you all come dressed in costume and ready 2/25!!!
Game of Thrones Conference Review
See below link of all the powerpoints and review questions. We barely got through half of the review questions that we made! So, plenty of material to chew on.
You have already completed the quiz before. Hence you can not start it again.
Quiz is loading...
You must sign in or sign up to start the quiz.
You have to finish following quiz, to start this quiz:
Results
0 of 10 questions answered correctly
Your time:
Time has elapsed
You have reached 0 of 0 points, (0)
Categories
Not categorized0%
Cardiovascular0%
1
2
3
4
5
6
7
8
9
10
Answered
Review
Question 1 of 10
1. Question
A 45-year-old man with end stage renal disease on hemodialysis and heart failure presents with acute shortness of breath. Vital signs are BP 188/104, HR 115, and oxygen saturation 93%. Physical examination reveals crackles bilaterally. Which of the following treatments should be initiated?
Correct
This patient presents with symptoms of acute decompensated heart failure and should be started on nitroglycerin therapy immediately. Patients present with shortness of breath, increased work of breathing, tachycardia, hypoxia, crackles on lung examination and jugular venous distension. These patients experience acute worsening of left ventricular function and output secondary to a number of mechanisms including increased systemic vascular resistance. Therapy focuses on reduction of preload to decrease the flow of blood into the lungs and afterload reduction to increased the effectiveness of the left ventricle. Both of these goals can be accomplished through the administration of nitroglycerin. At lower doses, nitroglycerin acts as a peripheral vasodilator and increases venous capacitance leading to decreased preload. At higher doses, nitroglycerin causes arterial vasodilation leading to decreased afterload. Because of its rapid onset of action, nitroglycerin is the first line medication in patients with ADHF.
Furosemide (A) may be useful in patients with volume overload and ADHF but this represents less than half of patients with ADHF. Additionally, the effects are delayed. Heparin (B) can be given in cases of ischemia induced ADHF but will not yield any immediate benefits. Morphine (C) was historically used as a preload reducer but has been associated with increased morbidity in patients with ADHF and is no longer recommended.
Incorrect
This patient presents with symptoms of acute decompensated heart failure and should be started on nitroglycerin therapy immediately. Patients present with shortness of breath, increased work of breathing, tachycardia, hypoxia, crackles on lung examination and jugular venous distension. These patients experience acute worsening of left ventricular function and output secondary to a number of mechanisms including increased systemic vascular resistance. Therapy focuses on reduction of preload to decrease the flow of blood into the lungs and afterload reduction to increased the effectiveness of the left ventricle. Both of these goals can be accomplished through the administration of nitroglycerin. At lower doses, nitroglycerin acts as a peripheral vasodilator and increases venous capacitance leading to decreased preload. At higher doses, nitroglycerin causes arterial vasodilation leading to decreased afterload. Because of its rapid onset of action, nitroglycerin is the first line medication in patients with ADHF.
Furosemide (A) may be useful in patients with volume overload and ADHF but this represents less than half of patients with ADHF. Additionally, the effects are delayed. Heparin (B) can be given in cases of ischemia induced ADHF but will not yield any immediate benefits. Morphine (C) was historically used as a preload reducer but has been associated with increased morbidity in patients with ADHF and is no longer recommended.
Question 2 of 10
2. Question
Which of the following statements is most accurate regarding acute ischemic heart disease?
Correct
A typical feature of acute coronary syndrome iscrushingretrosternal chest pain or pressure. Often this is lacking, and patients present with atypical features of the pain or the presence of angina equivalent symptoms (e.g., dyspnea, nausea, vomiting, dizziness). Many patients with a diagnosis of ACS have pain that is pleuritic, positional, or reproduced by palpation. One large study showed that up to 33% of patients diagnosed with acute myocardial infarction did not have chest pain on presentation. Atypical complaints include dyspnea;nausea;diaphoresis;syncope; and pain in the arms, epigastrium, shoulder, or neck.
Atypical features of ACS are present with increasing frequency in older populations. In patients older than 85 years (A), atypical symptoms are more common than typical chest pain, with dyspnea being the most common. Isolated physical exam findings are rarely diagnostic of the origin of chest pain. Palpation of the chest wall (B) may reveal localized tenderness, but 5%–10% of patients with ACS have chest pain and associated palpable chest wall tenderness. Being female (D) is a risk factor for an atypical presentation of ACS.
Incorrect
A typical feature of acute coronary syndrome iscrushingretrosternal chest pain or pressure. Often this is lacking, and patients present with atypical features of the pain or the presence of angina equivalent symptoms (e.g., dyspnea, nausea, vomiting, dizziness). Many patients with a diagnosis of ACS have pain that is pleuritic, positional, or reproduced by palpation. One large study showed that up to 33% of patients diagnosed with acute myocardial infarction did not have chest pain on presentation. Atypical complaints include dyspnea;nausea;diaphoresis;syncope; and pain in the arms, epigastrium, shoulder, or neck.
Atypical features of ACS are present with increasing frequency in older populations. In patients older than 85 years (A), atypical symptoms are more common than typical chest pain, with dyspnea being the most common. Isolated physical exam findings are rarely diagnostic of the origin of chest pain. Palpation of the chest wall (B) may reveal localized tenderness, but 5%–10% of patients with ACS have chest pain and associated palpable chest wall tenderness. Being female (D) is a risk factor for an atypical presentation of ACS.
Question 3 of 10
3. Question
A 52-year-old man with a history of erectile dysfunction presents to the Emergency Department with a complaint of “crushing” substernal chest pain. An electrocardiogram shows ST elevation in V2 through V4 with reciprocal depressions in the inferior leads. Which of the following is a contraindication to the use of nitroglycerin in patients with acute coronary syndrome?
Correct
Tadalafil use within the past 36 hours is a contraindication for nitroglycerin. Tadalafil is a phosphodiesterase inhibitors used in the treatment of erectile dysfunction. When co-administered with nitroglycerin, severe hypotension can occur. Its half-life is longer than that of sildenafil and vardenafil. Nitrates (e.g. nitroglycerin) breaks down into nitric oxide, which causes coronary vessel dilation and decreases myocardial ischemia. Phosphodiesterase inhibitors potentiate the effect of nitrates by preventing the breakdown of nitric oxide and can cause significant hypotension.
A suspect anteroseptal myocardial infarction (A) is not a contraindication. However, nitrates should be avoided in right ventricular infarcts due to the risk of hypotension. A systolic blood pressure of 115 mm Hg (B) is not contraindication to nitrates use. Sildenafil (D) is contraindicated less than 24 hours after last use.
Incorrect
Tadalafil use within the past 36 hours is a contraindication for nitroglycerin. Tadalafil is a phosphodiesterase inhibitors used in the treatment of erectile dysfunction. When co-administered with nitroglycerin, severe hypotension can occur. Its half-life is longer than that of sildenafil and vardenafil. Nitrates (e.g. nitroglycerin) breaks down into nitric oxide, which causes coronary vessel dilation and decreases myocardial ischemia. Phosphodiesterase inhibitors potentiate the effect of nitrates by preventing the breakdown of nitric oxide and can cause significant hypotension.
A suspect anteroseptal myocardial infarction (A) is not a contraindication. However, nitrates should be avoided in right ventricular infarcts due to the risk of hypotension. A systolic blood pressure of 115 mm Hg (B) is not contraindication to nitrates use. Sildenafil (D) is contraindicated less than 24 hours after last use.
Question 4 of 10
4. Question
Which of the following is NOT a method by which noninvasive ventilation modalities (such as BiPAP and CPAP) successfully treat patients in severe acute decompensated heart failure?
Correct
Noninvasive ventilation is a useful and powerful tool in treating acute decompensated heart failure. It has been shown to simultaneously decrease preload and afterload and therefore ameliorate the symptoms of heart failure. It also improves lung mechanics by recruiting atelectatic alveoli, increasing intrathoracic pressure, improving pulmonary compliance, and reducing the work of breathing. Noninvasive ventilation has also been shown to decrease endotracheal intubation rates, decrease the need for ICU admissions, and decrease mortality.
Incorrect
Noninvasive ventilation is a useful and powerful tool in treating acute decompensated heart failure. It has been shown to simultaneously decrease preload and afterload and therefore ameliorate the symptoms of heart failure. It also improves lung mechanics by recruiting atelectatic alveoli, increasing intrathoracic pressure, improving pulmonary compliance, and reducing the work of breathing. Noninvasive ventilation has also been shown to decrease endotracheal intubation rates, decrease the need for ICU admissions, and decrease mortality.
Question 5 of 10
5. Question
A 45-year-old woman without any significant past medical history presents to the emergency department with sudden-onset severe chest pain, which has resolved by the time she is evaluated. She has experienced this pattern of chest pain for several months and notes difficulty swallowing solids and liquids during these episodes. She denies any other associated symptoms. An ECG demonstrates normal sinus rhythm and serial troponin is negative. Which of the following will most likely reveal the underlying cause of the patient’s symptoms?
Correct
Distal esophageal spasm (formerly diffuse esophageal spasm) presents with sudden and severe chest pain and can present similarly to a myocardial infarction. The underlying pathophysiology is not well elucidated, however, it is believed to be associated with an overactivity of excitatory innervation or increased smooth muscle response to excitatory nerves. Patients with risk factors for coronary artery disease or an unclear presentation should have a cardiac etiology ruled out with an ECG and cardiac troponins. Specific historical factors that can point toward esophageal pathology include findings such as inability to swallow solids or liquids during these episodes. The diagnosis of diffuse esophageal spasm can be confirmed with manometry. Treatment includes management of GERD symptoms (if present), a calcium channel blocker such as diltiazem, or tricyclic antidepressants.
Incorrect
Distal esophageal spasm (formerly diffuse esophageal spasm) presents with sudden and severe chest pain and can present similarly to a myocardial infarction. The underlying pathophysiology is not well elucidated, however, it is believed to be associated with an overactivity of excitatory innervation or increased smooth muscle response to excitatory nerves. Patients with risk factors for coronary artery disease or an unclear presentation should have a cardiac etiology ruled out with an ECG and cardiac troponins. Specific historical factors that can point toward esophageal pathology include findings such as inability to swallow solids or liquids during these episodes. The diagnosis of diffuse esophageal spasm can be confirmed with manometry. Treatment includes management of GERD symptoms (if present), a calcium channel blocker such as diltiazem, or tricyclic antidepressants.
Question 6 of 10
6. Question
A previously healthy 48-year-old man presents to the emergency department with substernal chest pain for the past six hours. His electrocardiogram is shown. Your department is over two hours by air and four hours by ground transport from the nearest cardiac catheterization lab. Which of the following is the most appropriate management?
Correct
This patient has an ECG consistent with an anterior ST segment elevation myocardial infarction. Myocardial infarction occurs due to insufficient blood supply and lack of oxygen delivery most often secondary to ruptured coronary artery plaque and thrombus formation. Classic signs and symptoms of acute MI include chest pain radiating to either arm or the neck, nausea, dyspnea, and diaphoresis. The anterior wall is supplied by the left anterior descending artery. ST segment elevation in leads V3 and V4 is suggestive of an anterior wall infarct. Cardiac enzymes should be drawn and troponin I would characteristically be elevated in ST segment elevation myocardial infarction two to six hours after symptom onset. Lack of positive troponin should not delay treatment. ST segment elevation in two contiguous anatomic leads should prompt immediate initiation of therapy. Aspirin 324 mg PO chewable should be administered immediately to prevent further platelet aggregation. Clopidogrel and heparin are also indicated. Nitroglycerin may be given improve myocardial oxygen supply by dilating the coronary arteries; however, it is contraindicated in right ventricular infarct due to risk for profound hypotension. Definitive treatment for ST segment elevation myocardial infarction is cardiac catheterizationand revascularization. If time from medical contact to balloon time is going to be greater than 120 minutes, thrombolytics are recommended. While there is improvement in mortality with time to first medical contact to balloon time of less than 90 minutes compared to 120 minutes, the 2013 American College of Cardiology Foundation/American Heart Association recommends 120 minutes as an acceptable cut off for administering thrombolytics. This cut off is reasonable as presentation to a center without PCI available is a leading cause for delay in door to balloon time. The appropriate dosing of alteplase in ST segment elevation myocardial infarction is administration of alteplase 15 mg IV push followed by two subsequent alteplase infusions (0.75 mg/kg over 30 minutes and 0.5 mg/kg over 60 minutes). Arrangements for transfer should be made concurrently. Contraindications to alteplase should be reviewed before administration.
Administer intravenous atenolol and arrange for transfer (B) is incorrect. While beta-blockers are part of the management of coronary ischemia, the patient requires immediate thrombolysis. Transfer the patient via ground transport with alteplase available if patient deteriorates (C) is incorrect given that the patient is four hours away from the nearest cardiac catheterization lab by ground and alteplase should be given without delay. Transfer the patient via helicopter to the nearest cardiac catheterization lab (D) is correct if you can transfer the patient and have them in the cardiac catheterization lab within 120 minutes of first medical contact; however, your center is over two hours away by air, thus alteplase should be given.
contraindications to thrombolysis include (1) acute aortic dissection (confirmed or suspected), (2) active internal bleeding (excluding menses), (3) intracranial tumor, hemorrhage or arteriovenous malformation, (4) ischemic stroke within 3 months, (5) significant head or facial trauma within 3 months, or (6) a known allergy to the thrombolytic agent. Relative contraindications include (1) chronic or poorly controlled hypertension, (2) blood pressure > 180/110 mm Hg, (3) major surgery within 3 weeks, (4) internal bleeding within 2 to 4 weeks, (5) noncompressible vascular punctures, (6) pregnancy, (7) active peptic ulcer disease, and (8) current anticoagulation use.
Incorrect
This patient has an ECG consistent with an anterior ST segment elevation myocardial infarction. Myocardial infarction occurs due to insufficient blood supply and lack of oxygen delivery most often secondary to ruptured coronary artery plaque and thrombus formation. Classic signs and symptoms of acute MI include chest pain radiating to either arm or the neck, nausea, dyspnea, and diaphoresis. The anterior wall is supplied by the left anterior descending artery. ST segment elevation in leads V3 and V4 is suggestive of an anterior wall infarct. Cardiac enzymes should be drawn and troponin I would characteristically be elevated in ST segment elevation myocardial infarction two to six hours after symptom onset. Lack of positive troponin should not delay treatment. ST segment elevation in two contiguous anatomic leads should prompt immediate initiation of therapy. Aspirin 324 mg PO chewable should be administered immediately to prevent further platelet aggregation. Clopidogrel and heparin are also indicated. Nitroglycerin may be given improve myocardial oxygen supply by dilating the coronary arteries; however, it is contraindicated in right ventricular infarct due to risk for profound hypotension. Definitive treatment for ST segment elevation myocardial infarction is cardiac catheterizationand revascularization. If time from medical contact to balloon time is going to be greater than 120 minutes, thrombolytics are recommended. While there is improvement in mortality with time to first medical contact to balloon time of less than 90 minutes compared to 120 minutes, the 2013 American College of Cardiology Foundation/American Heart Association recommends 120 minutes as an acceptable cut off for administering thrombolytics. This cut off is reasonable as presentation to a center without PCI available is a leading cause for delay in door to balloon time. The appropriate dosing of alteplase in ST segment elevation myocardial infarction is administration of alteplase 15 mg IV push followed by two subsequent alteplase infusions (0.75 mg/kg over 30 minutes and 0.5 mg/kg over 60 minutes). Arrangements for transfer should be made concurrently. Contraindications to alteplase should be reviewed before administration.
Administer intravenous atenolol and arrange for transfer (B) is incorrect. While beta-blockers are part of the management of coronary ischemia, the patient requires immediate thrombolysis. Transfer the patient via ground transport with alteplase available if patient deteriorates (C) is incorrect given that the patient is four hours away from the nearest cardiac catheterization lab by ground and alteplase should be given without delay. Transfer the patient via helicopter to the nearest cardiac catheterization lab (D) is correct if you can transfer the patient and have them in the cardiac catheterization lab within 120 minutes of first medical contact; however, your center is over two hours away by air, thus alteplase should be given.
contraindications to thrombolysis include (1) acute aortic dissection (confirmed or suspected), (2) active internal bleeding (excluding menses), (3) intracranial tumor, hemorrhage or arteriovenous malformation, (4) ischemic stroke within 3 months, (5) significant head or facial trauma within 3 months, or (6) a known allergy to the thrombolytic agent. Relative contraindications include (1) chronic or poorly controlled hypertension, (2) blood pressure > 180/110 mm Hg, (3) major surgery within 3 weeks, (4) internal bleeding within 2 to 4 weeks, (5) noncompressible vascular punctures, (6) pregnancy, (7) active peptic ulcer disease, and (8) current anticoagulation use.
Question 7 of 10
7. Question
A 60-year-old man with hypertension and diabetes presents to the Emergency Department after a 20 minute episode of severe chest pain and dyspnea. He is currently asymptomatic. His ECG is shown. Stenosis of which of the following coronary arteries is responsible for his symptoms and ECG findings?
Correct
This patient is presenting with symptoms and an ECG consistent with Wellen’s syndrome which is highly specific for critical stenosis of the left anterior descending artery. Patients are at high risk for extensive anterior myocardial infarction within weeks to months. It is thought that patients have sudden occlusion of the LAD resulting in anginal symptoms and transient STEMI. Spontaneous reperfusion of the LAD results in resolution of symptoms and the classic findings on ECG. Patients are often asymptomatic when evaluated in the Emergency Department. The most common finding on ECG (found in 75% of cases) is deeply and symmetrically inverted T waves in the anterior precordial leads. Alternatively, biphasic T waves (initial positivity and terminal negativity) are seen in 25% of cases. The ECG findings are present when the patient is pain free. Cardiac markers are normal or mildly elevated. Patients should be admitted for cardiac catheterization given their high risk of infarction.
Wellen Syndrome
Highly specific for critical stenosis of the left anterior descending artery
ECG: deeply inverted or biphasic T waves in V2-3
May be pain free
Normal or minimally elevated troponin
Rx: urgent or emergent percutaneous coronary intervention
The circumflex artery (A) supplies the anterolateral portions of the heart. The left main coronary artery (C) gives rise to the left anterior descending artery and the circumflex artery. The right coronary artery (D) supplies the right ventricle and inferior portions of the heart. These arteries are not involved in Wellen’s syndrome.
Incorrect
This patient is presenting with symptoms and an ECG consistent with Wellen’s syndrome which is highly specific for critical stenosis of the left anterior descending artery. Patients are at high risk for extensive anterior myocardial infarction within weeks to months. It is thought that patients have sudden occlusion of the LAD resulting in anginal symptoms and transient STEMI. Spontaneous reperfusion of the LAD results in resolution of symptoms and the classic findings on ECG. Patients are often asymptomatic when evaluated in the Emergency Department. The most common finding on ECG (found in 75% of cases) is deeply and symmetrically inverted T waves in the anterior precordial leads. Alternatively, biphasic T waves (initial positivity and terminal negativity) are seen in 25% of cases. The ECG findings are present when the patient is pain free. Cardiac markers are normal or mildly elevated. Patients should be admitted for cardiac catheterization given their high risk of infarction.
Wellen Syndrome
Highly specific for critical stenosis of the left anterior descending artery
ECG: deeply inverted or biphasic T waves in V2-3
May be pain free
Normal or minimally elevated troponin
Rx: urgent or emergent percutaneous coronary intervention
The circumflex artery (A) supplies the anterolateral portions of the heart. The left main coronary artery (C) gives rise to the left anterior descending artery and the circumflex artery. The right coronary artery (D) supplies the right ventricle and inferior portions of the heart. These arteries are not involved in Wellen’s syndrome.
Question 8 of 10
8. Question
A 52 yo M comes to the ED with chest pain. You are handed the following EKG. Prior EKG shows LBBB. What is the most appropriate next step in management?
Correct
Sgarbossa criteria here is positive and activation of cath lab is indicated:
-Concardant ST depression: V2
-Concordant ST elevation: V5, V6
-Discordant ST elevation of over 25% of QRS complex: lead III, avF
Incorrect
Sgarbossa criteria here is positive and activation of cath lab is indicated:
-Concardant ST depression: V2
-Concordant ST elevation: V5, V6
-Discordant ST elevation of over 25% of QRS complex: lead III, avF
Question 9 of 10
9. Question
A 65-year-old woman presents with acute onset chest pain. Her husband died this morning and patient states she was in extreme distress. Her ECG initially shows ST elevations in leads V2-3 and she is taken for cardiac catheterization which demonstrates no evidence of obstructive disease, and cardiac echo shows reduced EF. She denies any use of illicit substances. Which of the following is true regarding this condition?
Correct
Takotsubo cardiomyopathy is also known as left apical ballooning or broken heart syndrome. Most commonly, patients are postmenopausal women who have just experienced significant emotional distress although there are numerous case reports from myriad other causes. It is unclear exactly why this occurs, but a sudden weakness in the myocardium develops after emotional distress possibly related to stress hormones, vascular spasm, focal myocarditis or other cellular changes. Patients develop symptoms consistent with acute coronary ischemia which most commonly include chest pain and dyspnea on exertion. The ECG is abnormal with ST segment elevations or deep T wave inversions usually on the anterior wall. Cardiac biomarkers are often positive. On cardiac catheterization, the coronary arteries do not have obstructive disease. If ventriculography or echocardiography is performed, the apex of the left ventricle is seen ballooning with an impaired ejection fraction. Prognosis is typically very good with recovery to normal wall motion and ejection fraction within a month.
Beta-blockers (A) do not change mortality in this condition. Almost all patients with takotsubo regain completely normal ejection fraction with no long term effects of the episode. Although beta-blockers and angiotensin converting enzyme inhibitors are considered mainstay therapy they do not impact mortality in these patients. AICD placement (B) is not indicated in this patient, as reduced EF is expected to naturally improve. Nitroglycerin (D) is not contraindicated in this patient. Nitroglycerin is unlikely to have any effect given the absence of coronary obstruction. In patients with hypertrophic cardiomyopathy and preload dependence for ventricular filling, agents that decrease preload like nitroglycerin should be avoided.
Incorrect
Takotsubo cardiomyopathy is also known as left apical ballooning or broken heart syndrome. Most commonly, patients are postmenopausal women who have just experienced significant emotional distress although there are numerous case reports from myriad other causes. It is unclear exactly why this occurs, but a sudden weakness in the myocardium develops after emotional distress possibly related to stress hormones, vascular spasm, focal myocarditis or other cellular changes. Patients develop symptoms consistent with acute coronary ischemia which most commonly include chest pain and dyspnea on exertion. The ECG is abnormal with ST segment elevations or deep T wave inversions usually on the anterior wall. Cardiac biomarkers are often positive. On cardiac catheterization, the coronary arteries do not have obstructive disease. If ventriculography or echocardiography is performed, the apex of the left ventricle is seen ballooning with an impaired ejection fraction. Prognosis is typically very good with recovery to normal wall motion and ejection fraction within a month.
Beta-blockers (A) do not change mortality in this condition. Almost all patients with takotsubo regain completely normal ejection fraction with no long term effects of the episode. Although beta-blockers and angiotensin converting enzyme inhibitors are considered mainstay therapy they do not impact mortality in these patients. AICD placement (B) is not indicated in this patient, as reduced EF is expected to naturally improve. Nitroglycerin (D) is not contraindicated in this patient. Nitroglycerin is unlikely to have any effect given the absence of coronary obstruction. In patients with hypertrophic cardiomyopathy and preload dependence for ventricular filling, agents that decrease preload like nitroglycerin should be avoided.
Question 10 of 10
10. Question
A 52-year-old man presents to the Emergency Department via ambulance with substernal chest pain. He received aspirin and nitroglycerin from emergency personnel in route. Vital signs include BP 95/55 mm Hg, HR 60 beats/minute, RR 20 breaths/minute, and T 97.6F. His electrocardiogram is shown. Which of the following is the most appropriate next diagnostic study?
Correct
This patient has an ECG consistent with an inferior ST segment elevation myocardial infarction. Inferior wall myocardial infarction may be accompanied by bradycardia due to involvement of the AV node or hypotension due to total right ventricular involvement. The inferior wall and right ventricle are supplied by the right coronary artery. ST segment elevation in leads II, III, and aVF is suggestive of an inferior wall infarct. This patient is suffering from hypotension and bradycardia as well, which suggest a potential right ventricular infarct. ECG findings suggestive of this include ST segment elevation in leads II, III, and aVF with the elevation in lead III greater than that of lead II or associated elevation in lead V1. Any ST segment elevation in the inferior leads should prompt a right-sided electrocardiogram. ST segment elevation in leads V4R, V5R and V6R is diagnostic of a right ventricular infarct. Cardiac enzymes should also be drawn and troponin I would characteristically be elevated in ST segment elevation myocardial infarction 2-6 hours after symptom onset. Lack of positive troponin should not delay treatment. ST segment elevation in two contiguous anatomic leads should prompt immediate initiation of therapy. Aspirin 325 mg PO chewable should be administered immediately to prevent further platelet aggregation. Clopidogrel and heparin are also indicated. Nitroglycerin may be given to improve myocardial oxygen supply by dilating the coronary arteries; however, it is contraindicated in right ventricular infarct due to risk for profound hypotension. This patient’s hypotension should be treated with IVF. Definitive treatment for ST segment elevation myocardial infarction is cardiac catheterization and revascularization. If the patient is going to be greater than 90 minutes from medical contact to balloon time from the nearest cardiac catheterization center, thrombolytics are recommended.
A chest radiograph (A) would be appropriate if you were concerned for occult pneumothorax or as an initial study to evaluate for widened mediastinum in aortic dissection. CT angiogram of the chest/abd (B) would be appropriate as a definitive study if you were concerned for aortic dissection, AAA, or pulmonary embolism. Posterior electrocardiogram (C) would be appropriate to evaluate for posterior ST segment elevation if you saw deep depression in leads V1 and V2 with prominent R waves.
Incorrect
This patient has an ECG consistent with an inferior ST segment elevation myocardial infarction. Inferior wall myocardial infarction may be accompanied by bradycardia due to involvement of the AV node or hypotension due to total right ventricular involvement. The inferior wall and right ventricle are supplied by the right coronary artery. ST segment elevation in leads II, III, and aVF is suggestive of an inferior wall infarct. This patient is suffering from hypotension and bradycardia as well, which suggest a potential right ventricular infarct. ECG findings suggestive of this include ST segment elevation in leads II, III, and aVF with the elevation in lead III greater than that of lead II or associated elevation in lead V1. Any ST segment elevation in the inferior leads should prompt a right-sided electrocardiogram. ST segment elevation in leads V4R, V5R and V6R is diagnostic of a right ventricular infarct. Cardiac enzymes should also be drawn and troponin I would characteristically be elevated in ST segment elevation myocardial infarction 2-6 hours after symptom onset. Lack of positive troponin should not delay treatment. ST segment elevation in two contiguous anatomic leads should prompt immediate initiation of therapy. Aspirin 325 mg PO chewable should be administered immediately to prevent further platelet aggregation. Clopidogrel and heparin are also indicated. Nitroglycerin may be given to improve myocardial oxygen supply by dilating the coronary arteries; however, it is contraindicated in right ventricular infarct due to risk for profound hypotension. This patient’s hypotension should be treated with IVF. Definitive treatment for ST segment elevation myocardial infarction is cardiac catheterization and revascularization. If the patient is going to be greater than 90 minutes from medical contact to balloon time from the nearest cardiac catheterization center, thrombolytics are recommended.
A chest radiograph (A) would be appropriate if you were concerned for occult pneumothorax or as an initial study to evaluate for widened mediastinum in aortic dissection. CT angiogram of the chest/abd (B) would be appropriate as a definitive study if you were concerned for aortic dissection, AAA, or pulmonary embolism. Posterior electrocardiogram (C) would be appropriate to evaluate for posterior ST segment elevation if you saw deep depression in leads V1 and V2 with prominent R waves.
Alas! We have arrived at the bread and butter of the cardio block. Activate that STEMI pager, push that nitro, and know that the troponins are oh so sensitive. We are talkin about chest pain, heart failure, and coronary artery disease. We will have FLIPs hosted by Drs. Praamsma, Yousif, and Maqbool. This will include an algorithm building station regarding an approach to chest pain, so make sure you do the required reading and keep in mind that all things that cause chest pressure aren’t coronary artery disease…NOW BUTTER UP THAT BACON
***NOTE: When taking the quiz, if you can’t see the pictures, RIGHT CLICK it and select “open link in new tab”. This won’t shut down your quiz and you will be able to see an expanded full size pic.***
*Required Material*
either read one of the following chps or listen to the below podcast
You have already completed the quiz before. Hence you can not start it again.
Quiz is loading...
You must sign in or sign up to start the quiz.
You have to finish following quiz, to start this quiz:
Results
0 of 10 questions answered correctly
Your time:
Time has elapsed
You have reached 0 of 0 points, (0)
Average score
Your score
Categories
Not categorized0%
1
2
3
4
5
6
7
8
9
10
Answered
Review
Question 1 of 10
1. Question
A 55-year old male with a history of hypertension and chronic kidney disease is brought in by his family for altered mental status and vomiting. They report he had been complaining of a headache over the past day and on the morning of presentation started to display bizarre behavior. On presentation, vitals are as follows: HR 105, BP 230/140, RR 16, Temp 98.6 F (37C). Physical exam is significant for altered mental status but is otherwise unremarkable. The patient has no focal neurologic deficits. CT head is negative. Which of the following is the most appropriate initial agent for the management of this patient’s likely condition?
Correct
Hypertensive emergency is defined as a markedly elevated blood pressure with evidence of acute cardiovascular, renal or neurologic end-organ damage. Rapid reduction of blood pressure is achieved with reduction of the mean arterial pressure (MAP) by 25-30%. Excessive reduction of blood pressure should be avoided as it may cause cerebral ischemia. The first-line agents for blood pressure reduction to consider are nitroprusside, nicardipine, or labetolol. Nicardipine affects both coronary and cerebral circulations and is a pure arterial vasodilator that prevents tachycardia, bradycardia and decreased preload. It reliably reduces blood pressure and is easy to titrate.
Incorrect
Hypertensive emergency is defined as a markedly elevated blood pressure with evidence of acute cardiovascular, renal or neurologic end-organ damage. Rapid reduction of blood pressure is achieved with reduction of the mean arterial pressure (MAP) by 25-30%. Excessive reduction of blood pressure should be avoided as it may cause cerebral ischemia. The first-line agents for blood pressure reduction to consider are nitroprusside, nicardipine, or labetolol. Nicardipine affects both coronary and cerebral circulations and is a pure arterial vasodilator that prevents tachycardia, bradycardia and decreased preload. It reliably reduces blood pressure and is easy to titrate.
Question 2 of 10
2. Question
A 55-year old male with a history of congestive heart failure presents with shortness of breath. Vital signs are: BP 220/150, HR 110, RR 35, O2 Sat 89% on room air. Which of the following is the most appropriate initial agent for blood pressure reduction?
Correct
The main indication for nitroglycerin is a patient with acute pulmonary edema who needs direct vasodilation. Nitroglycerin will also lower blood pressure, although not as quickly as nitroprusside. The other medications listed are not first-line agents as they will not quickly improve pulmonary edema. Nitroprusside is a potent arterial vasodilator that reduces afterload (instead of preload), is difficult to titrate, and may cause wide fluctuations in blood pressure. Labetolol is difficult to titrate, can cause wide fluctuations in blood pressure and is contraindicated in patients with congestive heart failure. Nicardipine is a pure arterial vasodilator.
Incorrect
The main indication for nitroglycerin is a patient with acute pulmonary edema who needs direct vasodilation. Nitroglycerin will also lower blood pressure, although not as quickly as nitroprusside. The other medications listed are not first-line agents as they will not quickly improve pulmonary edema. Nitroprusside is a potent arterial vasodilator that reduces afterload (instead of preload), is difficult to titrate, and may cause wide fluctuations in blood pressure. Labetolol is difficult to titrate, can cause wide fluctuations in blood pressure and is contraindicated in patients with congestive heart failure. Nicardipine is a pure arterial vasodilator.
Question 3 of 10
3. Question
Which of the following medications should NOT be given if the patient has been taking sildenafil?
Correct
The American Heart Association/American College of Cardiology (AHA/ACC) guidelines provide recommendations on the use of antihypertensive medications in unstable angina/non-ST-segment elevation MI. Nitroglycerin can be used to control both symptoms and BP; however, it should not be used to the exclusion of other therapies that are more likely to have a beneficial effect on outcomes. Patients should be asked if they have recently used sildenafil or one of its analogues, as the combination with nitrates can cause severe hypotension. The use of oral beta-blockers in the ED is optional. The current AHA/ACC guidelines suggest that oral beta-blockers can be given any time within the first 24 hours of presentation. Angiotensin-converting enzyme inhibitors and angiotensin receptor blockers may be used for patients with hypertension and left ventricular dysfunction or pulmonary congestion. Recommendations allow ACE inhibitors to be given within 24 hours of presentation.
Incorrect
The American Heart Association/American College of Cardiology (AHA/ACC) guidelines provide recommendations on the use of antihypertensive medications in unstable angina/non-ST-segment elevation MI. Nitroglycerin can be used to control both symptoms and BP; however, it should not be used to the exclusion of other therapies that are more likely to have a beneficial effect on outcomes. Patients should be asked if they have recently used sildenafil or one of its analogues, as the combination with nitrates can cause severe hypotension. The use of oral beta-blockers in the ED is optional. The current AHA/ACC guidelines suggest that oral beta-blockers can be given any time within the first 24 hours of presentation. Angiotensin-converting enzyme inhibitors and angiotensin receptor blockers may be used for patients with hypertension and left ventricular dysfunction or pulmonary congestion. Recommendations allow ACE inhibitors to be given within 24 hours of presentation.
Question 4 of 10
4. Question
A 62-year old female with a history of 3-vessel coronary artery bypass 2 years ago presents to the Emergency Department with 2 hours of acute substernal chest pain. The pain started suddenly while she was watching television. She is diaphoretic and complains of tearing pain that radiates to her left scapula. She vomited twice in the ambulance. Vitals signs include a blood pressure of 200/100 mmHg, heart rate of 120 beats/minute and a respiratory rate of 16 breaths/minute. Electrocardiogram reveals a sinus tachycardia with 2mm of ST elevation in the inferior leads. Chest x-ray is shown. Which of the following is the next best step in the management of this patient?
Correct
Aortic dissection is caused by a tear in the inner layer of the aorta, which allows blood to enter the wall and travel in a “false lumen”. Chest x-ray findings consistent with aortic dissection include a widened mediastinum, obscuration of aortic knob, presence of apical cap, lateral displacement of the trachea and depression of the left mainstem bronchus. ECG findings are variable and may depict an ST-Elevation myocardial infarction (MI) if a proximal dissection dissects into the coronary arteries. This is a rare entity that usually involves the right coronary artery, causing an inferior or posterior MI. This particular case is concerning for an ascending thoracic aortic dissection, whose treatment is surgical. However, while waiting for cardiothoracic surgical consult and radiographic imaging studies, acute control of the heart rate and blood pressure is imperative to minimize aortic wall stress and shearing. Initial acute treatment consists of an intravenous beta blocker to reduce the heart rate below 60 beats/min – while propranolol, labetalol, and esmolol can be used, esmolol has the advantage of a short half-life and use in patients with relative contraindications to beta-blockers (asthma, CHF). If systolic blood pressure remains >100mmHg despite beta-blockade, nitroprusside is classically recommended, although several other anti-hypertensive intravenous medications may be used.
Incorrect
Aortic dissection is caused by a tear in the inner layer of the aorta, which allows blood to enter the wall and travel in a “false lumen”. Chest x-ray findings consistent with aortic dissection include a widened mediastinum, obscuration of aortic knob, presence of apical cap, lateral displacement of the trachea and depression of the left mainstem bronchus. ECG findings are variable and may depict an ST-Elevation myocardial infarction (MI) if a proximal dissection dissects into the coronary arteries. This is a rare entity that usually involves the right coronary artery, causing an inferior or posterior MI. This particular case is concerning for an ascending thoracic aortic dissection, whose treatment is surgical. However, while waiting for cardiothoracic surgical consult and radiographic imaging studies, acute control of the heart rate and blood pressure is imperative to minimize aortic wall stress and shearing. Initial acute treatment consists of an intravenous beta blocker to reduce the heart rate below 60 beats/min – while propranolol, labetalol, and esmolol can be used, esmolol has the advantage of a short half-life and use in patients with relative contraindications to beta-blockers (asthma, CHF). If systolic blood pressure remains >100mmHg despite beta-blockade, nitroprusside is classically recommended, although several other anti-hypertensive intravenous medications may be used.
Question 5 of 10
5. Question
A 65-year-old female with a history of hypertension presents to the Emergency Department with severe tearing chest pain radiating to the upper back. BP 192/111, HR 125, RR 22, O2 Sat 100% on room air. Cardiac and lung examination are unremarkable, but you note a 1+ left radial artery pulse compared to 2+ right radial artery pulse. ECG is shown. In addition to appropriate consultation, which of the following is the most appropriate immediate next step in management?
Correct
This patient is presenting with symptoms concerning for acute aortic dissection. Patients with aortic dissection (specifically type A) can show ST elevations most commonly in the inferior leads due to involvement of the right coronary artery. In addition to cardiothoracic surgery consult, treatment of aortic dissection usually involves esmolol and nitroprusside; however, labetolol can be used in isolation. The most important treatment principle is to reduce the heart rate and then lower the blood pressure. Rate reduction is important in order to reduce shear stress on the aortic wall. As a beta blocker esmolol is effective in reducing the heart rate as it is easily titratable secondary to a short half-life. Nitroprusside is preferred to nitroglycerin as it is a more potent reducer of blood pressure, and it decreases afterload. Nitroprusside should not be used in isolation as it may increase the rate of rise of aortic wall pressure by increasing shearing forces. Reflex tachycardia may also result secondary to peripheral vasodilation increasing cardiac output.
Incorrect
This patient is presenting with symptoms concerning for acute aortic dissection. Patients with aortic dissection (specifically type A) can show ST elevations most commonly in the inferior leads due to involvement of the right coronary artery. In addition to cardiothoracic surgery consult, treatment of aortic dissection usually involves esmolol and nitroprusside; however, labetolol can be used in isolation. The most important treatment principle is to reduce the heart rate and then lower the blood pressure. Rate reduction is important in order to reduce shear stress on the aortic wall. As a beta blocker esmolol is effective in reducing the heart rate as it is easily titratable secondary to a short half-life. Nitroprusside is preferred to nitroglycerin as it is a more potent reducer of blood pressure, and it decreases afterload. Nitroprusside should not be used in isolation as it may increase the rate of rise of aortic wall pressure by increasing shearing forces. Reflex tachycardia may also result secondary to peripheral vasodilation increasing cardiac output.
Question 6 of 10
6. Question
A 55-year-old female with hypertension presents with sudden onset tearing chest pain radiating to her upper back. Vital signs are: BP 151/89, P 99, RR 18, O2Sat 99% room air, T 98.5F (36.9C). Physical exam reveals diminished bilateral femoral pulses. An image of the computed tomography angiography of the chest is shown. Morphine has resolved her pain. Labetalol is ordered and pending. What is the next best step in the management of this patient?
Correct
Aortic dissection is commonly seen in patients with long-term hypertension and connective tissue disorders, but can also be seen in pregnancy, coarctation of the aorta and a bicuspid aortic valve. Ascending aortic dissection is most common in the 50- to 60-year age range, whereas descending dissections occur more commonly in older individuals. Anatomic classification of aortic dissection is important for diagnosis and treatment. The Stanford classification system divides dissections into two types: A and B. Type A dissections involve the ascending aorta and Type B dissections involve the descending aorta.Type A dissections are more lethal, more common and require prompt surgical intervention. Commonly, Type A dissections often present with normotensive or hypotensive vitals, while Type B are hypertensive. The hypotension in Type A is usually due to cardiac tamponade, aortic rupture, or heart failure associated with severe aortic regurgitation. Pulse deficits are present only in 19% of Type A dissection and 9% of Type B dissection. Aortic regurgitation murmurs are present in 44% of Type A dissections and 12% of Type B dissections, according to the IRAAD registry (International Registry of Acute Aortic Dissection). While Type B dissections are typically treated medically, acute Type A ascending aortic dissections should be treated as a surgical emergency, given that these patients are at high risk for a life-threatening complications (e.g. aortic regurgitation, tamponade, and myocardial infarction) and high mortality rates for delayed repairs.
Incorrect
Aortic dissection is commonly seen in patients with long-term hypertension and connective tissue disorders, but can also be seen in pregnancy, coarctation of the aorta and a bicuspid aortic valve. Ascending aortic dissection is most common in the 50- to 60-year age range, whereas descending dissections occur more commonly in older individuals. Anatomic classification of aortic dissection is important for diagnosis and treatment. The Stanford classification system divides dissections into two types: A and B. Type A dissections involve the ascending aorta and Type B dissections involve the descending aorta.Type A dissections are more lethal, more common and require prompt surgical intervention. Commonly, Type A dissections often present with normotensive or hypotensive vitals, while Type B are hypertensive. The hypotension in Type A is usually due to cardiac tamponade, aortic rupture, or heart failure associated with severe aortic regurgitation. Pulse deficits are present only in 19% of Type A dissection and 9% of Type B dissection. Aortic regurgitation murmurs are present in 44% of Type A dissections and 12% of Type B dissections, according to the IRAAD registry (International Registry of Acute Aortic Dissection). While Type B dissections are typically treated medically, acute Type A ascending aortic dissections should be treated as a surgical emergency, given that these patients are at high risk for a life-threatening complications (e.g. aortic regurgitation, tamponade, and myocardial infarction) and high mortality rates for delayed repairs.
Question 7 of 10
7. Question
A 66-year male with a known 6 cm aortic aneurysm presents with sudden onset abdominal pain, hypotension and a palpable abdominal mass. What is the most common site that a aneurysm will rupture into?
Correct
All of the answer choices are sites that aortic aneurysms may rupture into, but aortic aneurysms most commonly rupture into the retroperitoneum. The most rapidly fatal location is the intraperitoneum. Less common sites of rupture include the gastrointestinal tract and the inferior vena cava.
Incorrect
All of the answer choices are sites that aortic aneurysms may rupture into, but aortic aneurysms most commonly rupture into the retroperitoneum. The most rapidly fatal location is the intraperitoneum. Less common sites of rupture include the gastrointestinal tract and the inferior vena cava.
Question 8 of 10
8. Question
What is the most important factor determining the risk of aortic aneurysm rupture?
Correct
The most common factor predicting the risk of rupture is the size of the aneurysm. Aneurysms occur when a segment of the aorta is weakened, and the larger the aneurysm, the greater tension exerted on the wall. Most ruptured aneurysms are greater than 5cm. There is a high incidence of aneurysms in patients with atherosclerotic disease and men older than 65 years of age. Other risk factors include history of smoking, hypertension, and family history of abdominal aortic aneurysm.
Incorrect
The most common factor predicting the risk of rupture is the size of the aneurysm. Aneurysms occur when a segment of the aorta is weakened, and the larger the aneurysm, the greater tension exerted on the wall. Most ruptured aneurysms are greater than 5cm. There is a high incidence of aneurysms in patients with atherosclerotic disease and men older than 65 years of age. Other risk factors include history of smoking, hypertension, and family history of abdominal aortic aneurysm.
Question 9 of 10
9. Question
A 64-year-old man with a history of hypertension presents to the Emergency Department requesting medication refills. He states that he has not taken his medications for the last 2 weeks. His blood pressure is 190/100. He has no complaints at this time. He has prescription bottles for atenolol and hydrochlorothiazide. What management is indicated?
Correct
This patient presents with asymptomatic hypertension in the setting of medical non-compliance and should berestarted on his medications and scheduled for follow up with a primary care physician. Accelerated hypertension is defined as markedly elevated blood pressure in the absence of symptoms. This is in contrast with hypertensive emergency where the patient has symptoms or evidence of end organ system dysfunction or both as a result of elevated blood pressure. Accelerated hypertension has a poor long-term prognosis if not controlled but does not pose an immediate threat. As such, it should not be aggressively treated with parenteral medications. Rapid lowering of blood pressure in patients with chronic elevated blood pressure can cause organ hypoperfusion, particularly brain hypoperfusion, and lead to serious sequelae. These patients should be restarted on their medications (if appropriate) and sent for follow up with a primary care physician to monitor and treat the elevated blood pressure.
Incorrect
This patient presents with asymptomatic hypertension in the setting of medical non-compliance and should berestarted on his medications and scheduled for follow up with a primary care physician. Accelerated hypertension is defined as markedly elevated blood pressure in the absence of symptoms. This is in contrast with hypertensive emergency where the patient has symptoms or evidence of end organ system dysfunction or both as a result of elevated blood pressure. Accelerated hypertension has a poor long-term prognosis if not controlled but does not pose an immediate threat. As such, it should not be aggressively treated with parenteral medications. Rapid lowering of blood pressure in patients with chronic elevated blood pressure can cause organ hypoperfusion, particularly brain hypoperfusion, and lead to serious sequelae. These patients should be restarted on their medications (if appropriate) and sent for follow up with a primary care physician to monitor and treat the elevated blood pressure.
Question 10 of 10
10. Question
Nitroprusside is a medication that should be avoided in which of the following hypertensive situations?
Correct
Hypertensive encephalopathy describes reversible cerebral disorders associated with high BP in the absence of cerebral thrombosis or hemorrhage. The theoretical mechanism of hypertensive encephalopathy is a rapid rise in BP that overwhelms the autoregulatory mechanisms of the brain and leads to blood-brain barrier permeability and brain edema. The symptoms of hypertensive encephalopathy can include headache, seizures, visual disturbances, nausea, and vomiting. The diagnosis must be made only after other potential hypertensive emergencies are excluded. A PubMed search for clinical trials, meta-analyses, and randomized controlled trials of hypertensive encephalopathy yielded 22 articles. None of the trials dealt directly with treatment or prognosis, and no studies suggested which agent is best for short-term reduction of BP in hypertensive encephalopathy. However, nitroprusside should be avoided in patients with this disorder, as the drug has been shown to decrease systemic pressure while preserving intracranial perfusion pressures. In the absence of data, the consensus goal of treatment is often stated as a 20% to 25% reduction in mean arterial pressure or a DBP of 100 to 110 mg Hg.
Incorrect
Hypertensive encephalopathy describes reversible cerebral disorders associated with high BP in the absence of cerebral thrombosis or hemorrhage. The theoretical mechanism of hypertensive encephalopathy is a rapid rise in BP that overwhelms the autoregulatory mechanisms of the brain and leads to blood-brain barrier permeability and brain edema. The symptoms of hypertensive encephalopathy can include headache, seizures, visual disturbances, nausea, and vomiting. The diagnosis must be made only after other potential hypertensive emergencies are excluded. A PubMed search for clinical trials, meta-analyses, and randomized controlled trials of hypertensive encephalopathy yielded 22 articles. None of the trials dealt directly with treatment or prognosis, and no studies suggested which agent is best for short-term reduction of BP in hypertensive encephalopathy. However, nitroprusside should be avoided in patients with this disorder, as the drug has been shown to decrease systemic pressure while preserving intracranial perfusion pressures. In the absence of data, the consensus goal of treatment is often stated as a 20% to 25% reduction in mean arterial pressure or a DBP of 100 to 110 mg Hg.
We continue on with cardiology! This week the FLIPs will be done by Drs. Koripella, Saker, and Guignard! In addition, we will have Dr. Berk’s EKG rounds, an M&M done by myself, and Journal Club by Drs. Jones and Inman!
Also specific reading for Dr. Koripella’s station: Paul, Marik, and Racquel Rivera. “Hypertensive emergencies: an update.” https://emcrit.org/wp-content/uploads/2011/12/htn.pdf
You have already completed the quiz before. Hence you can not start it again.
Quiz is loading...
You must sign in or sign up to start the quiz.
You have to finish following quiz, to start this quiz:
Results
0 of 10 questions answered correctly
Your time:
Time has elapsed
You have reached 0 of 0 points, (0)
Categories
Not categorized0%
Cardiovascular0%
Neurology0%
1
2
3
4
5
6
7
8
9
10
Answered
Review
Question 1 of 10
1. Question
EKG findings that are associated with poor short-term outcomes in patients with syncope include all of the following EXCEPT:
Correct
Although the definition of abnormal ECG varies among the many studies examining their role in the diagnosis of syncope, particular attention should be paid to any non-sinus rhythm, signs of ischemia, or conduction abnormalities.
Red flags to look for include:
Any non-sinus rhythm
signs of ischemia (ST or T wave abnormalities)
conduction abnormalities
Delta waves for WPW
Prolong QT
First degree heartblock, and Mobitz type I are NOT associated with poor outcomes in syncope
Incorrect
Although the definition of abnormal ECG varies among the many studies examining their role in the diagnosis of syncope, particular attention should be paid to any non-sinus rhythm, signs of ischemia, or conduction abnormalities.
Red flags to look for include:
Any non-sinus rhythm
signs of ischemia (ST or T wave abnormalities)
conduction abnormalities
Delta waves for WPW
Prolong QT
First degree heartblock, and Mobitz type I are NOT associated with poor outcomes in syncope
Question 2 of 10
2. Question
A 61-yo man is brought to the ED after an episode of chest pain. His initial electrocardiogram shows a sinus rhythm with ST-segment depression in the anterior leads. He later reports palpitations, but otherwise feels fine. Blood pressure is 132/86 mm Hg. A repeat electrocardiogram is shown. Which of the following is the most appropriate treatment?
Correct
The patient has ventricular tachycardia (heart rate > 100 beats/minute originating from an ectopic ventricular focus). Electrocardiographic hallmarks of monomorphic VT include a rapid, regular rhythm with a wide QRS complex > 120 milliseconds with consistent beat-to-beat morphology. P waves are not seen, other than an occasional dissociated P wave. VT can be nonsustained, occurring with a few ventricular beats at a time which terminate spontaneously, or can occur in a sustained fashion.
VT occurs most commonly in the setting of ischemic heart disease/MI, but can also be seen in cardiomyopathies, valvular heart disease, inherited ion channel disorders, and drug toxicity. Hypoxia and electrolyte disorders, such as hyperkalemia, increase the propensity for ventricular ectopy and VT. The clinical effects of VT vary widely. Pulseless VT, the most severe manifestation, requires immediate defibrillation/ACLS. Unstable patients in VT who have a pulse, as evidenced by hypotension, ischemic chest pain, or altered mental status, should undergo electrical cardioversion. This patient, who has a normal blood pressure and minimal symptoms, has stable VT. Pharmacologic agents are first-line therapy for stable VT. Treatment options include procainamide, amiodarone, and lidocaine. Elective cardioversion can be performed if the patient fails to convert with antiarrhythmics or becomes clinically unstable. Administration of intravenous adenosine (A) is the treatment for supraventricular tachycardia. Defibrillation (C) is indicated in pulseless ventricular tachycardia, a form of cardiac arrest. Electrical cardioversion (D) is the treatment for unstable ventricular tachycardia, or if he fails to convert with pharmacologic therapy.
Incorrect
The patient has ventricular tachycardia (heart rate > 100 beats/minute originating from an ectopic ventricular focus). Electrocardiographic hallmarks of monomorphic VT include a rapid, regular rhythm with a wide QRS complex > 120 milliseconds with consistent beat-to-beat morphology. P waves are not seen, other than an occasional dissociated P wave. VT can be nonsustained, occurring with a few ventricular beats at a time which terminate spontaneously, or can occur in a sustained fashion.
VT occurs most commonly in the setting of ischemic heart disease/MI, but can also be seen in cardiomyopathies, valvular heart disease, inherited ion channel disorders, and drug toxicity. Hypoxia and electrolyte disorders, such as hyperkalemia, increase the propensity for ventricular ectopy and VT. The clinical effects of VT vary widely. Pulseless VT, the most severe manifestation, requires immediate defibrillation/ACLS. Unstable patients in VT who have a pulse, as evidenced by hypotension, ischemic chest pain, or altered mental status, should undergo electrical cardioversion. This patient, who has a normal blood pressure and minimal symptoms, has stable VT. Pharmacologic agents are first-line therapy for stable VT. Treatment options include procainamide, amiodarone, and lidocaine. Elective cardioversion can be performed if the patient fails to convert with antiarrhythmics or becomes clinically unstable. Administration of intravenous adenosine (A) is the treatment for supraventricular tachycardia. Defibrillation (C) is indicated in pulseless ventricular tachycardia, a form of cardiac arrest. Electrical cardioversion (D) is the treatment for unstable ventricular tachycardia, or if he fails to convert with pharmacologic therapy.
Question 3 of 10
3. Question
A 40-year-old man presents to the ED with nausea and vomiting for 3 days. He feels improved after treatment with IV fluids and prochlorperazine. One hour later, he complains of palpitations and lightheadedness. Vital signs are BP 100/60 mm Hg, HR 170, and pulse oximetry 96% on room air. The patient’s rhythm strip is shown. Which of the following is the most appropriate next step in management?
Correct
The patient’s rhythm strip demonstrates torsades de pointes, a polymorphic ventricular tachycardia precipitated by QT interval prolongation. Torsades de pointes is french for “twisting of the points,” which refers to the undulating appearance of the QRS complex. If untreated, this rhythm can lead to ventricular fibrillation. An intravenous bolus of magnesium sulfate is considered the first-line treatment for torsades de pointes. QT interval prolongation can be congenital, acquired, or a combination of both. The QT interval represents the sum of the action potential duration of the ventricular cardiomyocytes. The cardiac action potential during depolarization is characterized by inward sodium and calcium currents. During repolarization, the inward calcium current decreases and an outward potassium current increases. Drugs can prolong the QT interval by blocking or prolonging these currents. Antiemetics such as prochlorperazine are among the many different medications that can cause QT interval prolongation. Defibrillation is indicated in ventricular fibrillation or pulseless ventricular tachycardia, it is not considered first line for torsades de pointes, but is indicated if patient is pulseless. Adenosine is the treatment for SVT. Synchronized cardioversion is not indicated here, however overdrive pacing is indicated in IV magnesium resistant torsades if the patient remains stable.
Drugs that prolong QT: phenothiazine, abx, cyclic antidepressants, class IA antiarrhythmics (procainamide, quinidine), class IC (flecanide), droperidol, methadone, cocaine
Electrolyte abnormalities that prolong QT: hypomag, hypoCa, hypoK
Incorrect
The patient’s rhythm strip demonstrates torsades de pointes, a polymorphic ventricular tachycardia precipitated by QT interval prolongation. Torsades de pointes is french for “twisting of the points,” which refers to the undulating appearance of the QRS complex. If untreated, this rhythm can lead to ventricular fibrillation. An intravenous bolus of magnesium sulfate is considered the first-line treatment for torsades de pointes. QT interval prolongation can be congenital, acquired, or a combination of both. The QT interval represents the sum of the action potential duration of the ventricular cardiomyocytes. The cardiac action potential during depolarization is characterized by inward sodium and calcium currents. During repolarization, the inward calcium current decreases and an outward potassium current increases. Drugs can prolong the QT interval by blocking or prolonging these currents. Antiemetics such as prochlorperazine are among the many different medications that can cause QT interval prolongation. Defibrillation is indicated in ventricular fibrillation or pulseless ventricular tachycardia, it is not considered first line for torsades de pointes, but is indicated if patient is pulseless. Adenosine is the treatment for SVT. Synchronized cardioversion is not indicated here, however overdrive pacing is indicated in IV magnesium resistant torsades if the patient remains stable.
Drugs that prolong QT: phenothiazine, abx, cyclic antidepressants, class IA antiarrhythmics (procainamide, quinidine), class IC (flecanide), droperidol, methadone, cocaine
Electrolyte abnormalities that prolong QT: hypomag, hypoCa, hypoK
Question 4 of 10
4. Question
Which of the following medications is contraindicated in treating ventricular escape rhythms?
Correct
In this scenario, the ventricle is acting as the pacemaker for the heart, so this tissue is the last line of defense for the heart to provide any sort of electrical activity to maintain cardiac output. Lidocaine, which may abolish the ventricular rhythm completely, is contraindicated because it may cause cardiac standstill. Atropine, due to its vagolytic properties, enhances sinus node automaticity and AV nodal conduction. Isoproterenol, a beta-adrenergic agonist, has both inotropic and chronotropic effects. Isoproterenol increases myocardial oxygen demand and should be used with caution in ischemic myocardium. Glucagon has been shown to be useful in the treatment of bradyarrhythmias secondary to beta-adrenergic blocking agents and calcium antagonists. Glucagon stimulates the SA node directly giving some mild increase in heart rate. Glucagon also increases cardiac contractility.
Incorrect
In this scenario, the ventricle is acting as the pacemaker for the heart, so this tissue is the last line of defense for the heart to provide any sort of electrical activity to maintain cardiac output. Lidocaine, which may abolish the ventricular rhythm completely, is contraindicated because it may cause cardiac standstill. Atropine, due to its vagolytic properties, enhances sinus node automaticity and AV nodal conduction. Isoproterenol, a beta-adrenergic agonist, has both inotropic and chronotropic effects. Isoproterenol increases myocardial oxygen demand and should be used with caution in ischemic myocardium. Glucagon has been shown to be useful in the treatment of bradyarrhythmias secondary to beta-adrenergic blocking agents and calcium antagonists. Glucagon stimulates the SA node directly giving some mild increase in heart rate. Glucagon also increases cardiac contractility.
Question 5 of 10
5. Question
A magnet placed over a standard pacemaker will cause
Correct
Placement of a magnet over a pacemaker will cause synchronous pacing at model-specific rates, it does NOT turn off the pacemaker.
Of note, AICDs all have pacemaker capability (usually from the R ventricular lead), and magnets DISABLE the AICD shocking ability, but it DEFAULTS the device to a pacemaker mode. So a magnet never over an AICD turns off the defibrillator and converts it to a pacemaker mode (usually 60bpm)
Incorrect
Placement of a magnet over a pacemaker will cause synchronous pacing at model-specific rates, it does NOT turn off the pacemaker.
Of note, AICDs all have pacemaker capability (usually from the R ventricular lead), and magnets DISABLE the AICD shocking ability, but it DEFAULTS the device to a pacemaker mode. So a magnet never over an AICD turns off the defibrillator and converts it to a pacemaker mode (usually 60bpm)
Question 6 of 10
6. Question
An 81-year-old woman presents to the emergency department with malaise and SOB for 1 day. According to her daughter, she worsened over the last hour and now has mental status changes that cause her to not respond as quickly. She has a history of HTN and a prior MI 5 years ago. Vital signs show HR 30 bpm, BP 90/60 mm Hg, RR 20/min, and oxygen saturation 95% on room air. The rhythm strip is shown. What is the most appropriate initial treatment for this patient?
Correct
The patient in this question is presenting with a story and electrocardiogram that is consistent with third-degree atrioventricular heart block. In a third-degree (complete) atrioventricular heart block, no atrial impulses reach the ventricle. More than half of cases are caused by idiopathic progressive cardiac conduction disease with myocardial fibrosis and sclerosis that affects the conduction system. Other causes include myocardial ischemia, myocarditis, endocarditis, and atrioventricular nodal blocking medications. Patients generally present with fatigue, dyspnea, chest pain, syncope, mental status changes, or cardiac arrest. It is important for the clinician to obtain a good history including a list of all medications to determine the most likely etiology of the complete heart block. Diagnosis is usually confirmed with an electrocardiogram. Initial management depends on whether the patient is hemodynamically stable or unstable. Signs of hemodynamic instability include chest pain, mental status changes, acute pulmonary edema, and hypotension. This patient has mental status changes and is hypotensive. Steps should immediately be taken to prepare for transcutaneous cardiac pacing, but in the meantime, the patient should be treated with atropine. Atropine may only be successful in approximately 30% of patients with third-degree heart block, so other medications may be required, but the most recent Advanced Cardiac Life Support guidelines recommend atropine 0.5 mg intravenously as initial therapy.
Calcium gluconate (B) would be recommended in any patient suspected of having hyperkalemia leading to a cardiac dysrhythmia. This patient’s history does not suggest hyperkalemia, and typically bradycardia associated with hyperkalemia presents with a wide complex rhythm instead of a narrow complex rhythm on electrocardiogram. Dobutamine (C) is recommended for patients with complete heart block and congestive heart failure. However, other medications are usually recommended before using dobutamine. Metoprolol (D) is a beta blocker and would worsen the patient’s heart block
Incorrect
The patient in this question is presenting with a story and electrocardiogram that is consistent with third-degree atrioventricular heart block. In a third-degree (complete) atrioventricular heart block, no atrial impulses reach the ventricle. More than half of cases are caused by idiopathic progressive cardiac conduction disease with myocardial fibrosis and sclerosis that affects the conduction system. Other causes include myocardial ischemia, myocarditis, endocarditis, and atrioventricular nodal blocking medications. Patients generally present with fatigue, dyspnea, chest pain, syncope, mental status changes, or cardiac arrest. It is important for the clinician to obtain a good history including a list of all medications to determine the most likely etiology of the complete heart block. Diagnosis is usually confirmed with an electrocardiogram. Initial management depends on whether the patient is hemodynamically stable or unstable. Signs of hemodynamic instability include chest pain, mental status changes, acute pulmonary edema, and hypotension. This patient has mental status changes and is hypotensive. Steps should immediately be taken to prepare for transcutaneous cardiac pacing, but in the meantime, the patient should be treated with atropine. Atropine may only be successful in approximately 30% of patients with third-degree heart block, so other medications may be required, but the most recent Advanced Cardiac Life Support guidelines recommend atropine 0.5 mg intravenously as initial therapy.
Calcium gluconate (B) would be recommended in any patient suspected of having hyperkalemia leading to a cardiac dysrhythmia. This patient’s history does not suggest hyperkalemia, and typically bradycardia associated with hyperkalemia presents with a wide complex rhythm instead of a narrow complex rhythm on electrocardiogram. Dobutamine (C) is recommended for patients with complete heart block and congestive heart failure. However, other medications are usually recommended before using dobutamine. Metoprolol (D) is a beta blocker and would worsen the patient’s heart block
Question 7 of 10
7. Question
A patient is brought into the ED by EMS as a STEMI activation and promptly loses his pulse and becomes unresponsive. The monitor shows ventricular fibrillation. Which of the following describes the correct sequence of treatment, assuming the patient is already connected to a defibrillator?
Correct
As per the 2010 AHA guidelines, CPR should only take place until the defibrillator is ready, and defibrillation at 200 J should be performed as soon as possible in VF arrest. Escalating doses of 50–100–150 J are no longer recommended and 200 J should be used for biphasic defibrillators. Though epinephrine is recommended as part of ACLS, it should not take precedence over defibrillation and has not shown long-term benefit in the treatment of cardiac arrest.
Incorrect
As per the 2010 AHA guidelines, CPR should only take place until the defibrillator is ready, and defibrillation at 200 J should be performed as soon as possible in VF arrest. Escalating doses of 50–100–150 J are no longer recommended and 200 J should be used for biphasic defibrillators. Though epinephrine is recommended as part of ACLS, it should not take precedence over defibrillation and has not shown long-term benefit in the treatment of cardiac arrest.
Question 8 of 10
8. Question
An 88 yo woman with a h/o HTN presents to the ED with palpitations and SOB for one week. She has intermittent mild chest pain but denies any current chest pain. She takes metoprolol for her hypertension and is compliant with her daily dose. Vital signs show HR 146 bpm, BP 106/68 mm Hg, RR 12/min, and T 37.4°C. She has an unremarkable physical examination aside from tachycardia. An ECG is shown. What is the most appropriate treatment at this time?
Correct
this ECG demonstrates a narrow complex irregular tachycardia that is consistent with atrial fibrillation with rapid ventricular response. Patients with atrial fibrillation with a rapid ventricular rate should have the rate controlled to prevent worsening symptoms such as dyspnea and chest pain and development of a cardiomyopathy. In the past, physicians preferred a rhythm control strategy when treating atrial fibrillation with rapid ventricular response. However, multiple studies have not shown a mortality benefit to rhythm control versus rate control, thus, a rate control treatment strategy is preferred. The clinician also needs to consider the urgency of therapy when choosing the appropriate treatment. In patients with clinical or hemodynamic compromise, immediate cardioversion may be required. The patient in this question has mild symptoms, but none currently, and she is not hypotensive. She is an appropriate candidate for pharmacologic treatment. There are several treatment options to control the ventricular rate in atrial fibrillation, but beta-blockers and calcium channel blockers remain superior to other options like digoxin. Anecdotally, emergency physicians prefer calcium channel blockers because they find them to be more effective in treating acute atrial fibrillation with rapid ventricular response, however, both beta-blockers and calcium channel blockers have been shown to be equally effective in the acute setting. Since this patient is already taking metoprolol for other reasons, it might be wise for the clinician to use intravenous metoprolol at this time.
Adenosine (A) is an atrioventricular nodal blocking agent that is indicated to convert paroxysmal supraventricular tachycardia to sinus rhythm. When a patient presents with a fast ventricular rhythm that is difficult to distinguish between atrial fibrillation and supraventricular tachycardia, adenosine may also be used to determine the underlying rhythm. The clinician should be able to recognize this patient’s rhythm as irregular, rather than a regular narrow complex tachycardia. Amiodarone (B) is an antidysrhythmic that can be used to slow the ventricular rate in atrial fibrillation with rapid ventricular response, and it causes less hypotension than calcium channel blockers, but due to its negative long-term side effects, it is not used as first-line therapy. It is used more often for a wide complex tachycardia suggestive of ventricular tachycardia. Intravenous fluid administration (C) would be indicated for patients with sinus tachycardia thought to be due to infection or dehydration. This patient’s rhythm is not regular and does not suggest sinus tachycardia.
Incorrect
this ECG demonstrates a narrow complex irregular tachycardia that is consistent with atrial fibrillation with rapid ventricular response. Patients with atrial fibrillation with a rapid ventricular rate should have the rate controlled to prevent worsening symptoms such as dyspnea and chest pain and development of a cardiomyopathy. In the past, physicians preferred a rhythm control strategy when treating atrial fibrillation with rapid ventricular response. However, multiple studies have not shown a mortality benefit to rhythm control versus rate control, thus, a rate control treatment strategy is preferred. The clinician also needs to consider the urgency of therapy when choosing the appropriate treatment. In patients with clinical or hemodynamic compromise, immediate cardioversion may be required. The patient in this question has mild symptoms, but none currently, and she is not hypotensive. She is an appropriate candidate for pharmacologic treatment. There are several treatment options to control the ventricular rate in atrial fibrillation, but beta-blockers and calcium channel blockers remain superior to other options like digoxin. Anecdotally, emergency physicians prefer calcium channel blockers because they find them to be more effective in treating acute atrial fibrillation with rapid ventricular response, however, both beta-blockers and calcium channel blockers have been shown to be equally effective in the acute setting. Since this patient is already taking metoprolol for other reasons, it might be wise for the clinician to use intravenous metoprolol at this time.
Adenosine (A) is an atrioventricular nodal blocking agent that is indicated to convert paroxysmal supraventricular tachycardia to sinus rhythm. When a patient presents with a fast ventricular rhythm that is difficult to distinguish between atrial fibrillation and supraventricular tachycardia, adenosine may also be used to determine the underlying rhythm. The clinician should be able to recognize this patient’s rhythm as irregular, rather than a regular narrow complex tachycardia. Amiodarone (B) is an antidysrhythmic that can be used to slow the ventricular rate in atrial fibrillation with rapid ventricular response, and it causes less hypotension than calcium channel blockers, but due to its negative long-term side effects, it is not used as first-line therapy. It is used more often for a wide complex tachycardia suggestive of ventricular tachycardia. Intravenous fluid administration (C) would be indicated for patients with sinus tachycardia thought to be due to infection or dehydration. This patient’s rhythm is not regular and does not suggest sinus tachycardia.
Question 9 of 10
9. Question
Which of the following is TRUE regarding a patient with syncope?
Correct
Brief (usually less than 10 seconds) tonic–clonic seizure activity can accompany syncope of any etiology. This activity is not accompanied by postictal disorientation, and it does not represent true seizure activity. It is usually described as myoclonic jerking. For cerebrovascular disease to cause a loss of consciousness, either both cerebral hemispheres or the brainstem must be deprived of blood flow. Therefore transient ischemic attacks and stroke are rarely the cause of syncope. Screening laboratory studies have been shown to add little to establishing a cause of syncope. In most cases, hypoglycemia is clinically suspected and abnormal electrolytes rarely account for a loss of consciousness. Anemia from bleeding is usually clinically evident. In otherwise healthy individuals, syncope is most commonly idiopathic (50%).
Incorrect
Brief (usually less than 10 seconds) tonic–clonic seizure activity can accompany syncope of any etiology. This activity is not accompanied by postictal disorientation, and it does not represent true seizure activity. It is usually described as myoclonic jerking. For cerebrovascular disease to cause a loss of consciousness, either both cerebral hemispheres or the brainstem must be deprived of blood flow. Therefore transient ischemic attacks and stroke are rarely the cause of syncope. Screening laboratory studies have been shown to add little to establishing a cause of syncope. In most cases, hypoglycemia is clinically suspected and abnormal electrolytes rarely account for a loss of consciousness. Anemia from bleeding is usually clinically evident. In otherwise healthy individuals, syncope is most commonly idiopathic (50%).
Question 10 of 10
10. Question
A 30 yo healthy man presents to the ED with palpitations that began suddenly 1 hour prior to presentation. He has no associated lightheadedness, chest pain, or shortness of breath. His vital signs are T 98.4°F, BP 110/70, HR 170, RR 18, and O2 sat 99% on room air. ECG is shown. Which of the following is the most appropriate initial therapy?
Correct
The patient’s ECG shows atrial fibrillation (AF) and an especially rapid ventricular response (RVR). Its variable, bizarre, wide QRS complexes suggest the presence of preexcited – or the Wolff-Parkinson-White (WPW) syndrome-related – AF. In hemodynamically stable patients, the initial treatment of preexcited AF with RVR consists of rhythm control with an antidysrhythmic agent such as procainamide 100 mg IV. While rate control with AV nodal blocking agents (e.g. diltiazem, metoprolol) is generally the initial treatment for AF with RVR, these medications’ effects can be disastrous for patients with preexcited AF. In this condition, rapidly conducting accessory pathways exist that can carry atrial impulses to the ventricle at rates exceeding 250 beats per minute. AV nodal blocking agents cause both faster and preferential conduction through these accessory pathways, which can result in extremely rapid ventricular response rates and deterioration to ventricular fibrillation. For these reasons, AV nodal blocking agents are contraindicated in preexcited AF.
Adenosine (A) is a short-acting AV nodal blocking agent. While useful in the management of narrow-complex, regular tachydysrhythmias such as AV nodal reentrant tachycardia, it has no role in the management of AF with RVR. Furthermore, its use is contraindicated in preexcited AF. While the initial treatment for AF with RVR generally consists of rate control with IV calcium channel blockers, such as diltiazem (B), or beta blockers such as metoprolol, use of these medications is contraindicated in preexcited AF. Synchronized electrical cardioversion (D) is indicated in the management of a number of tachydysrhythmias, including hemodynamically unstable AF with RVR. However initial treatment with pharmacologic therapy is appropriate for hemodynamically stable AF with RVR.
Incorrect
The patient’s ECG shows atrial fibrillation (AF) and an especially rapid ventricular response (RVR). Its variable, bizarre, wide QRS complexes suggest the presence of preexcited – or the Wolff-Parkinson-White (WPW) syndrome-related – AF. In hemodynamically stable patients, the initial treatment of preexcited AF with RVR consists of rhythm control with an antidysrhythmic agent such as procainamide 100 mg IV. While rate control with AV nodal blocking agents (e.g. diltiazem, metoprolol) is generally the initial treatment for AF with RVR, these medications’ effects can be disastrous for patients with preexcited AF. In this condition, rapidly conducting accessory pathways exist that can carry atrial impulses to the ventricle at rates exceeding 250 beats per minute. AV nodal blocking agents cause both faster and preferential conduction through these accessory pathways, which can result in extremely rapid ventricular response rates and deterioration to ventricular fibrillation. For these reasons, AV nodal blocking agents are contraindicated in preexcited AF.
Adenosine (A) is a short-acting AV nodal blocking agent. While useful in the management of narrow-complex, regular tachydysrhythmias such as AV nodal reentrant tachycardia, it has no role in the management of AF with RVR. Furthermore, its use is contraindicated in preexcited AF. While the initial treatment for AF with RVR generally consists of rate control with IV calcium channel blockers, such as diltiazem (B), or beta blockers such as metoprolol, use of these medications is contraindicated in preexcited AF. Synchronized electrical cardioversion (D) is indicated in the management of a number of tachydysrhythmias, including hemodynamically unstable AF with RVR. However initial treatment with pharmacologic therapy is appropriate for hemodynamically stable AF with RVR.
Ohhhhhh boy, Cardio block is HERE! The excitement is palpable, your heart is a flutter, you could faint at the mere thought of educational goodness right around the corner (though we all know that the most common cause of syncope is in fact…idiopathic). Truly, this will be a special conference. We have Drs. Darr and Moore running FLIPs on syncope and a procedure lab on pacing! Also, Roberto will rouse from his mid morning siesta to run his first FLIP ever on dysrhythmias!
*Required Material*
Review video on transvenous pacemaking (choose 1 of the 3)
You have already completed the quiz before. Hence you can not start it again.
Quiz is loading...
You must sign in or sign up to start the quiz.
You have to finish following quiz, to start this quiz:
Results
0 of 10 questions answered correctly
Your time:
Time has elapsed
You have reached 0 of 0 points, (0)
Categories
Not categorized0%
1
2
3
4
5
6
7
8
9
10
Answered
Review
Question 1 of 10
1. Question
A 22-year old female presents to the Emergency Department with two episodes of sudden onset left lower quadrant pain, nausea and vomiting. The first episode lasted for a few hours and spontaneously resolved for a few hours before returning again. After administration of pain medications, her pain has improved although she still feels “achy” in the left lower quadrant. She is afebrile with a white blood cell count of 11.0, and her physical exam is significant for mild left lower quadrant tenderness without rebound or guarding. Bedside urine pregnancy test and urine dipstick are both negative. Pelvic ultrasound demonstrates a 5.4cm simple left ovarian cyst with normal arterial blood flow but decreased venous flow compared to the right ovary. What is the most appropriate next step in management?
Correct
This patient is presenting with ovarian torsion. This patient’s cyst is greater than 5cm, putting her at risk for ovarian torsion. Her history of episodes of sudden onset pain is concerning for stuttering, intermittent torsion leading up to this event. Although ultrasound demonstrates intact arterial blood flow, the most frequent ultrasonographic abnormality in ovarian torsion is either decreased or absence of venous flow in the presence of intact arterial flow. Laparoscopy is the gold standard for diagnosis and management.
Incorrect
This patient is presenting with ovarian torsion. This patient’s cyst is greater than 5cm, putting her at risk for ovarian torsion. Her history of episodes of sudden onset pain is concerning for stuttering, intermittent torsion leading up to this event. Although ultrasound demonstrates intact arterial blood flow, the most frequent ultrasonographic abnormality in ovarian torsion is either decreased or absence of venous flow in the presence of intact arterial flow. Laparoscopy is the gold standard for diagnosis and management.
Question 2 of 10
2. Question
A 18-year-old girl with no previous medical history, presents with suprapubic pain with nausea. She denies urinary frequency, urgency or dysuria. She is currently sexually active with 1 male partner. Pelvic exam shows yellow-green frothy vaginal discharge, and punctate hemorrhage around cervix. Which of the following is TRUE regarding this condition?
Correct
Trichomonas vaginalis, a protozoa, is the causative agent of trichomoniasis. It is the most common non-viral sexually transmitted infection worldwide. Patients typically complain of yellow-green, frothy and malodorous vaginal discharge, with protozoa seen on wet mount. “Strawberry cervix”, or punctate hemorrhage around cervix, is seen on exam. Vaginal pH becomes more alkalotic, and is generally greater than 4.5. Treatment of trichomonas vaginitis is metronidazole. Clue cell is seen in bacterial vaginosis. Recent antibiotics use is a common risk factor for candidal vaginitis.
Incorrect
Trichomonas vaginalis, a protozoa, is the causative agent of trichomoniasis. It is the most common non-viral sexually transmitted infection worldwide. Patients typically complain of yellow-green, frothy and malodorous vaginal discharge, with protozoa seen on wet mount. “Strawberry cervix”, or punctate hemorrhage around cervix, is seen on exam. Vaginal pH becomes more alkalotic, and is generally greater than 4.5. Treatment of trichomonas vaginitis is metronidazole. Clue cell is seen in bacterial vaginosis. Recent antibiotics use is a common risk factor for candidal vaginitis.
Question 3 of 10
3. Question
A 65-year old female presents to the Emergency Room with a chief complaint of vaginal bleeding for 5 days. She is using about 2 pads per day. Prior to this episode, she has not had a menstrual period for 9 years. She has no past medical or surgical history. Vital signs are normal and her hemoglobin is 12.5 g/dL. Pelvic exam reveals a scant amount of dried blood in the vaginal vault, with mildly atrophic vaginal mucosa but no lesions. The uterus is of appropriate size, and there is no cervical motion tenderness or adnexal tenderness. What is the next best step in management of this patient?
Correct
The most common causes of postmenopausal vaginal bleeding is vaginal/endometrial atrophy 60%) and endometrial polyps (12%). However, endometrial cancer comprises about 10% of incidence. Given the stability of the patient, no further emergent imaging is indicated at this time, and urgent outpatient gynecology referral for further workup, including, but not limited to, endometrial biopsy, cervical cytology, and/or transvaginal ultraosund.
First line treatment of symptomatic atrophic vaginitis is vaginal moisturizing agents and lubricants. If that fails, and there is no contraindication for hormonal therapy (such as estrogen-based tumors like breast cancer), then low dose vaginal estrogen is the next step. In this question, the patient is stable and first-line therapy is nonhormonal moisturizing/lubricating agents and outpatient gynecology referral for endometrial biopsy, cervical cytology, and/or ultrasound to exclude endometrial cancer first. The biopsy should be obtained BEFORE starting any treatment. While the workup for vaginal bleeding may include serum testing, there is no indication with this clinically stable and otherwise normal patient to emergently order blood tests. These tests, along with other imaging or biopsy/cytology testing, may be performed on an outpatient basis.
Incorrect
The most common causes of postmenopausal vaginal bleeding is vaginal/endometrial atrophy 60%) and endometrial polyps (12%). However, endometrial cancer comprises about 10% of incidence. Given the stability of the patient, no further emergent imaging is indicated at this time, and urgent outpatient gynecology referral for further workup, including, but not limited to, endometrial biopsy, cervical cytology, and/or transvaginal ultraosund.
First line treatment of symptomatic atrophic vaginitis is vaginal moisturizing agents and lubricants. If that fails, and there is no contraindication for hormonal therapy (such as estrogen-based tumors like breast cancer), then low dose vaginal estrogen is the next step. In this question, the patient is stable and first-line therapy is nonhormonal moisturizing/lubricating agents and outpatient gynecology referral for endometrial biopsy, cervical cytology, and/or ultrasound to exclude endometrial cancer first. The biopsy should be obtained BEFORE starting any treatment. While the workup for vaginal bleeding may include serum testing, there is no indication with this clinically stable and otherwise normal patient to emergently order blood tests. These tests, along with other imaging or biopsy/cytology testing, may be performed on an outpatient basis.
Question 4 of 10
4. Question
Which of the following is the most common ultrasound finding for patients with ovarian torsion?
Correct
An ultrasound exam is usually the initial diagnostic study in the workup for ovarian torsion. The most common ultrasound finding in ovarian torsion is enlargement of the ovary. Enlargement develops due to impaired venous and lymphatic drainage, in addition to edema and hemorrhage that may occur. Less common findings include identification of a twisted pedicle (whirlpool sign), free pelvic fluid, and identification of an ovarian mass. RISK FACTORS: ovarian mass >5mm, reproductive age, pregnancy, ovulation induction, prior torsion. CLINICAL: adnexal pain/mass, vomiting, fever, vaginal bleeding
Free pelvic and intraperitoneal fluid (B) may surround the twisted ovary. This is usually the result of interstitial fluid that weeps off an affected ovary rather than true rupture of the capsule. Many cases of surgically proven ovarian torsion will have documented blood flow (C) on Doppler exam because the ovary has a dual blood supply from both the ovarian and uterine arteries. In addition, torsion is often intermittent, so findings may vary, depending on the time of the exam. Identification of an ovarian mass or cyst (>4 cm) (D) may suggest the diagnosis of ovarian torsion, but it is not the most common finding on ultrasound.
Incorrect
An ultrasound exam is usually the initial diagnostic study in the workup for ovarian torsion. The most common ultrasound finding in ovarian torsion is enlargement of the ovary. Enlargement develops due to impaired venous and lymphatic drainage, in addition to edema and hemorrhage that may occur. Less common findings include identification of a twisted pedicle (whirlpool sign), free pelvic fluid, and identification of an ovarian mass. RISK FACTORS: ovarian mass >5mm, reproductive age, pregnancy, ovulation induction, prior torsion. CLINICAL: adnexal pain/mass, vomiting, fever, vaginal bleeding
Free pelvic and intraperitoneal fluid (B) may surround the twisted ovary. This is usually the result of interstitial fluid that weeps off an affected ovary rather than true rupture of the capsule. Many cases of surgically proven ovarian torsion will have documented blood flow (C) on Doppler exam because the ovary has a dual blood supply from both the ovarian and uterine arteries. In addition, torsion is often intermittent, so findings may vary, depending on the time of the exam. Identification of an ovarian mass or cyst (>4 cm) (D) may suggest the diagnosis of ovarian torsion, but it is not the most common finding on ultrasound.
Question 5 of 10
5. Question
A 32-year-old woman presents with pain and swelling in the vaginal area. Examination reveals the finding below. What management is indicated?
Correct
This patient presents with a Bartholin’s abscess and should have incision and drainage (I+D) performed with the incision on the mucosal surface. Bartholin’s abscesses are infections located in the Bartholin’s glands which lie inferiorly to the vaginal opening. Patients develop cysts of the gland that become secondarily infected. These abscesses typically are caused by normally occurring aerobic and anaerobic bacteria in the vagina but may also be caused by sexually transmitted infections. Patients present with swelling and pain near the labium. Examination revels a tender, fluctuant mass along the posterolateral margin of the vaginal vestibule. Treatment focuses on incision and drainage with insertion of a Word catheter. The Word catheter has a small balloon at the end that is inflated after insertion and remains in place for 6 to 8 weeks. Because of this duration, the incision should be made on the mucosal surface so that the Word catheter can be tucked into the vaginal opening for patient comfort. Incision and drainage is usually adequate but patients with overlying cellulitis may require antibiotics. After discharge, patients should perform sitz baths to aid with drainage. Recurrence is common.
Incorrect
This patient presents with a Bartholin’s abscess and should have incision and drainage (I+D) performed with the incision on the mucosal surface. Bartholin’s abscesses are infections located in the Bartholin’s glands which lie inferiorly to the vaginal opening. Patients develop cysts of the gland that become secondarily infected. These abscesses typically are caused by normally occurring aerobic and anaerobic bacteria in the vagina but may also be caused by sexually transmitted infections. Patients present with swelling and pain near the labium. Examination revels a tender, fluctuant mass along the posterolateral margin of the vaginal vestibule. Treatment focuses on incision and drainage with insertion of a Word catheter. The Word catheter has a small balloon at the end that is inflated after insertion and remains in place for 6 to 8 weeks. Because of this duration, the incision should be made on the mucosal surface so that the Word catheter can be tucked into the vaginal opening for patient comfort. Incision and drainage is usually adequate but patients with overlying cellulitis may require antibiotics. After discharge, patients should perform sitz baths to aid with drainage. Recurrence is common.
Question 6 of 10
6. Question
A 22-year-old woman presents with lower abdominal pain and vaginal discharge. She is sexually active with men with inconsistent barrier protection. Her vitals are normal other than temperature of 101°F. On examination, there is yellow cervical discharge, no cervical motion tenderness, but uterine and left adnexal tenderness. An ultrasound does not show any evidence of tubo-ovarian abscess. What is the most appropriate treatment?
Correct
This patient has a clinical presentation consistent with pelvic inflammatory disease (PID). PID is an ascending infection that begins in the vagina or cervix. In the sexually active female, the most common responsible organisms are Chlamydia trachomatis and Neisseria gonorrhoeae. Frequently, the infection is polymicrobial. The most common presenting symptom is lower abdominal pain. Patients may also develop fever, vaginal discharge, dyspareunia or abnormal bleeding. On physical examination, the patient typically has a fever and is tender on pelvic examination either in the lower abdomen over the uterus, on cervical motion or in the adnexa. The absence of cervical motion tenderness does not rule out PID and the CDC recommends empiric treatment for sexually active women presenting with lower abdominal pain and one of the following if no other cause is identified: cervical motion tenderness, adnexal tenderness or uterine tenderness. For outpatient management, patients are treated with ceftriaxone 250 mg IM followed by a two-week course of doxycycline. Metronidazole is sometimes added to the regimen at the judgment of the clinician.
Incorrect
This patient has a clinical presentation consistent with pelvic inflammatory disease (PID). PID is an ascending infection that begins in the vagina or cervix. In the sexually active female, the most common responsible organisms are Chlamydia trachomatis and Neisseria gonorrhoeae. Frequently, the infection is polymicrobial. The most common presenting symptom is lower abdominal pain. Patients may also develop fever, vaginal discharge, dyspareunia or abnormal bleeding. On physical examination, the patient typically has a fever and is tender on pelvic examination either in the lower abdomen over the uterus, on cervical motion or in the adnexa. The absence of cervical motion tenderness does not rule out PID and the CDC recommends empiric treatment for sexually active women presenting with lower abdominal pain and one of the following if no other cause is identified: cervical motion tenderness, adnexal tenderness or uterine tenderness. For outpatient management, patients are treated with ceftriaxone 250 mg IM followed by a two-week course of doxycycline. Metronidazole is sometimes added to the regimen at the judgment of the clinician.
Question 7 of 10
7. Question
A 43-year old non-pregnant female presents to the Emergency Department with acute onset, severe vaginal bleeding. Initial vital signs: HR 125, BP 85/50, RR 26. Multiple units of blood products are empirically being administered with crystalloid fluids while pending laboratory blood studies. Examination of the vagina is severely limited secondary to large amounts of exsanguination, so the vaginal canal is packed. Repeat vital signs are: HR 145, BP 76/45, RR 30, and the patient is feeling increasingly anxious and lightheaded. Obstetric/Gynecology and Interventional radiology have been consulted. Which of the following is the next best step in management of this patient?
Correct
The correct answer is IV estrogens. High-dose estrogen is thought to promote rapid regrowth of endometrium and stabilize uterine bleeding within the first five hours of administration. In hemodynamically unstable patients, IV estrogen is recommended, while oral estrogen is appropriate for hemodynamically stable patients. Oxytocin and methylergonovine can be used in post-partum bleeding.
Carbaprost tromethamine is a prostaglandin analog used in postpartum bleeding that stimulates uterine contractility, promoting hemostasis at the placental site. Methylergonovine is used in post-partum uterine bleeding, by increasing uterine smooth muscle contractions to reduce blood loss. Recombinant factor VIIa has been FDA-approved for use in bleeding in patients with hemophilia A/B, factor VII deficiency, or acquired hemophilia. Off-label, recombinant factor VIIa has been used as a general hemostatic agent – in this patient, IV estrogen should be first utilized before moving onto more controversial, last-ditch efforts.
Incorrect
The correct answer is IV estrogens. High-dose estrogen is thought to promote rapid regrowth of endometrium and stabilize uterine bleeding within the first five hours of administration. In hemodynamically unstable patients, IV estrogen is recommended, while oral estrogen is appropriate for hemodynamically stable patients. Oxytocin and methylergonovine can be used in post-partum bleeding.
Carbaprost tromethamine is a prostaglandin analog used in postpartum bleeding that stimulates uterine contractility, promoting hemostasis at the placental site. Methylergonovine is used in post-partum uterine bleeding, by increasing uterine smooth muscle contractions to reduce blood loss. Recombinant factor VIIa has been FDA-approved for use in bleeding in patients with hemophilia A/B, factor VII deficiency, or acquired hemophilia. Off-label, recombinant factor VIIa has been used as a general hemostatic agent – in this patient, IV estrogen should be first utilized before moving onto more controversial, last-ditch efforts.
Question 8 of 10
8. Question
A 45-year-old female presents to the ER with abdominal pain and increased abdominal girth. She denies EtOH, smoking, or drug use and has no past medical history. Physical exam is significant for a distended abdomen with a fluid wave. CT scan reveals a pelvic mass with carcinomatosis. What lab test is likely to support the diagnosis?
Correct
This patient likely has ovarian cancer and the biomarker likely to support this diagnosis is CA-125. AFP is elevated in certain germ cell tumors as well as in Hepatocellular CA. CEA is elevated in colorectal CA. CA 19-9 is elevated in pancreatic and some types of colorectal CA.
Incorrect
This patient likely has ovarian cancer and the biomarker likely to support this diagnosis is CA-125. AFP is elevated in certain germ cell tumors as well as in Hepatocellular CA. CEA is elevated in colorectal CA. CA 19-9 is elevated in pancreatic and some types of colorectal CA.
Question 9 of 10
9. Question
Which of the following is the most likely etiology of Fitz-Hugh-Curtis syndrome?
Correct
Fitz-Hugh-Curtis syndrome is a condition that occurs in the setting of pelvic inflammatory disease (PID) and results in inflammation of the capsule surrounding the liver and the peritoneal surface of the anterior abdominal wall. It occurs in about 10% of patients with PID. Although it can be caused by any organisms responsible for pelvic inflammatory disease, Chlamydia trachomatis is most often implicated. Patients present with right upper quadrant pleuritic pain and tenderness. They may also have symptoms of PID, such as pelvic pain and vaginal discharge although these symptoms may be mild or lacking. Treatment regimens are similar to those for PID.
nfection with Gardnerella vaginalis (B) results in symptoms of vaginitis, but does not play a role in the development of Fitz-Hugh-Curtis syndrome. Hepatitis C virus (C) causes hepatitis, but is also not involved in the development of Fitz-Hugh-Curtis syndrome. Neisseria gonorrhoeae (D) can cause Fitz-Hugh-Curtis syndrome although it is more likely to be due to a C. trachomatis.
Incorrect
Fitz-Hugh-Curtis syndrome is a condition that occurs in the setting of pelvic inflammatory disease (PID) and results in inflammation of the capsule surrounding the liver and the peritoneal surface of the anterior abdominal wall. It occurs in about 10% of patients with PID. Although it can be caused by any organisms responsible for pelvic inflammatory disease, Chlamydia trachomatis is most often implicated. Patients present with right upper quadrant pleuritic pain and tenderness. They may also have symptoms of PID, such as pelvic pain and vaginal discharge although these symptoms may be mild or lacking. Treatment regimens are similar to those for PID.
nfection with Gardnerella vaginalis (B) results in symptoms of vaginitis, but does not play a role in the development of Fitz-Hugh-Curtis syndrome. Hepatitis C virus (C) causes hepatitis, but is also not involved in the development of Fitz-Hugh-Curtis syndrome. Neisseria gonorrhoeae (D) can cause Fitz-Hugh-Curtis syndrome although it is more likely to be due to a C. trachomatis.
Question 10 of 10
10. Question
A 6-year-old child presents to the ED accompanied her mother complaining of vaginal discharge for the last 7 days. The mother describes it as malodorous and today she noted small specks of blood in the child’s underwear. The child began attending school several weeks ago. She has no past medical history and has otherwise been in good health. Which of the following is the most likely diagnosis?
Correct
Vaginal foreign bodies can manifest as vaginal discharge. The discharge associated with a foreign body is often malodorous and bloody or dark brown in color and occurs daily. Potential foreign bodies include small pieces of toilet paper and small objects or toys. In this case, the child recently started attending school and is likely toileting by herself. As a result, she may be at risk of poor hygiene and potentially may have a small piece of toilet paper stuck within the vagina. Attempted manual removal can be performed on cooperative children over 7 years of age through irrigation with normal saline. Vaginoscopy under anesthesia in the operating room may be necessary in younger children.
Incorrect
Vaginal foreign bodies can manifest as vaginal discharge. The discharge associated with a foreign body is often malodorous and bloody or dark brown in color and occurs daily. Potential foreign bodies include small pieces of toilet paper and small objects or toys. In this case, the child recently started attending school and is likely toileting by herself. As a result, she may be at risk of poor hygiene and potentially may have a small piece of toilet paper stuck within the vagina. Attempted manual removal can be performed on cooperative children over 7 years of age through irrigation with normal saline. Vaginoscopy under anesthesia in the operating room may be necessary in younger children.
This week we are covering gynecologic complaints that are not related to pregnancy. FLIPs will be done by Drs. Inman, Moore, and White/Maqbool. This will be followed by oral boards done by Drs. Liu and McElroy, admin curriculum updates, and session #2 on wellness covering work-life balance.

















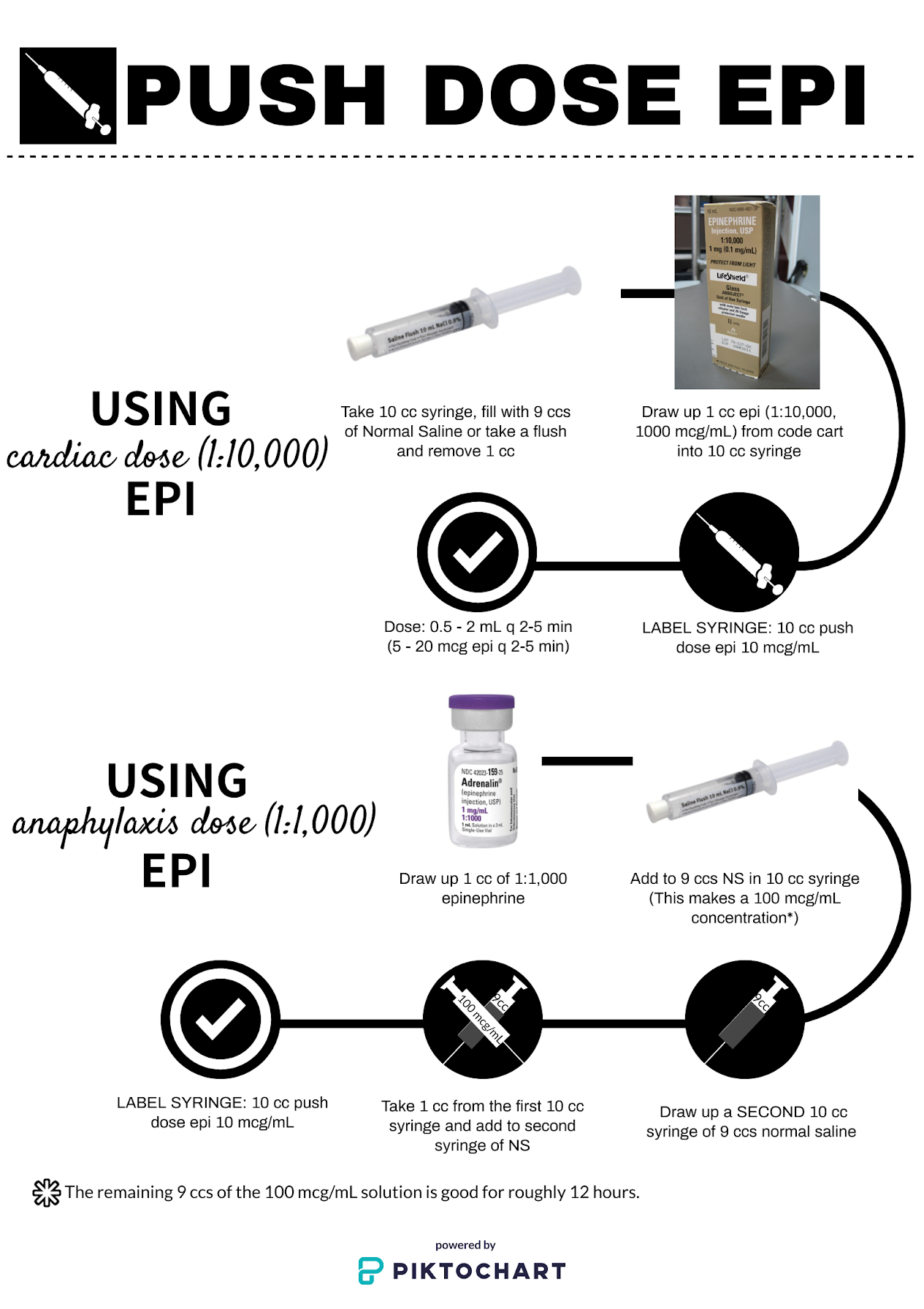{kind=link}
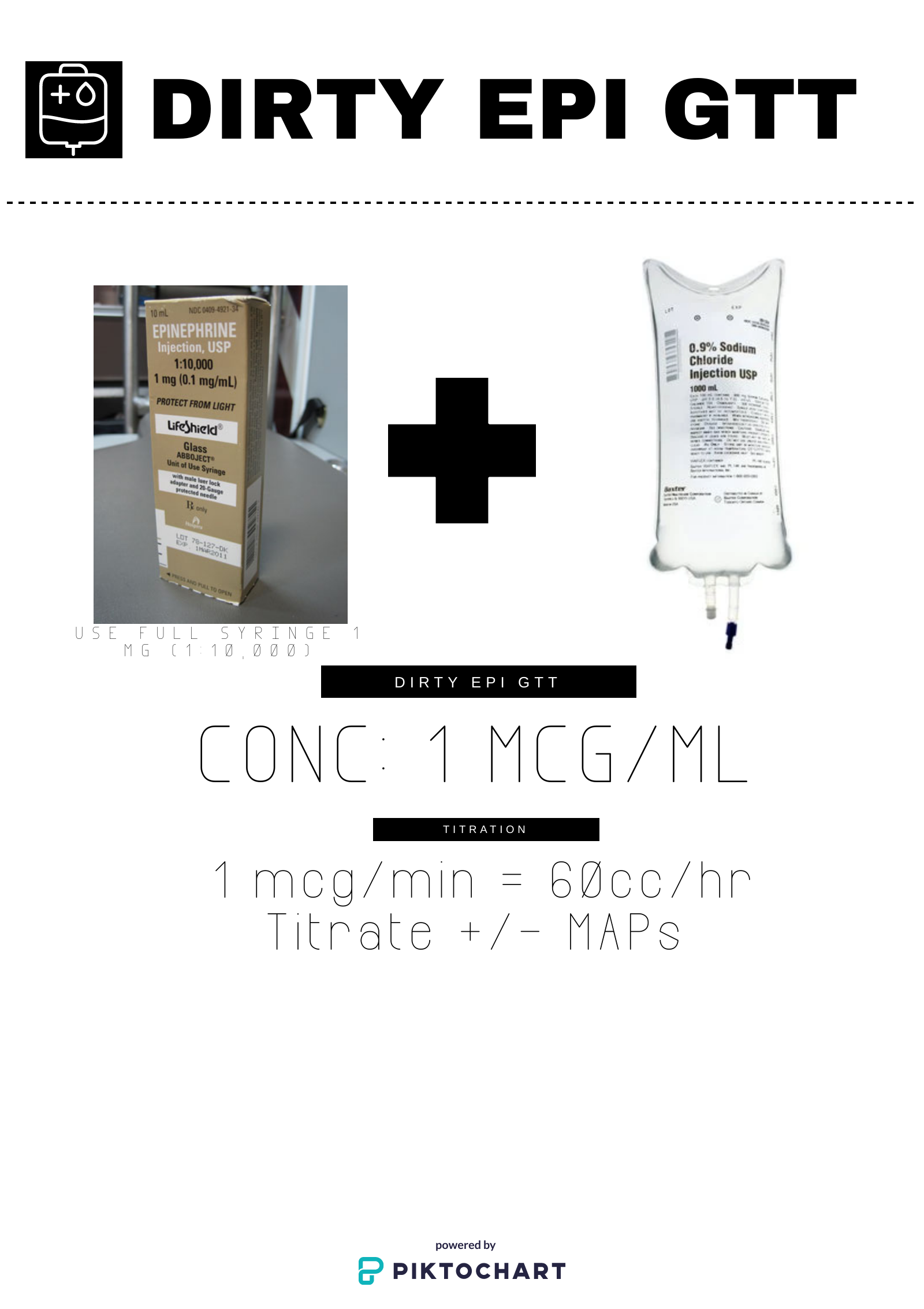{kind=link}